
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-056
Stent-Λ-Balloon Technique for the Treatment of LAD Ostial Stenosis
By Mutlu Vural, Emirhan Hancıoglu, Ishak Yılmaz
Presenter
Emirhan Hancıoglu
Authors
Mutlu Vural1, Emirhan Hancıoglu2, Ishak Yılmaz2
Affiliation
Private clinic, Turkey1, Sbu Bagcılar Training and Research Hospital, Turkey2,
View Study Report
TCTAP C-056
CORONARY - Bifurcation/Left Main Diseases and Intervention
Stent-Λ-Balloon Technique for the Treatment of LAD Ostial Stenosis
Mutlu Vural1, Emirhan Hancıoglu2, Ishak Yılmaz2
Private clinic, Turkey1, Sbu Bagcılar Training and Research Hospital, Turkey2,
Clinical Information
Patient initials or Identifier Number
İK
Relevant Clinical History and Physical Exam
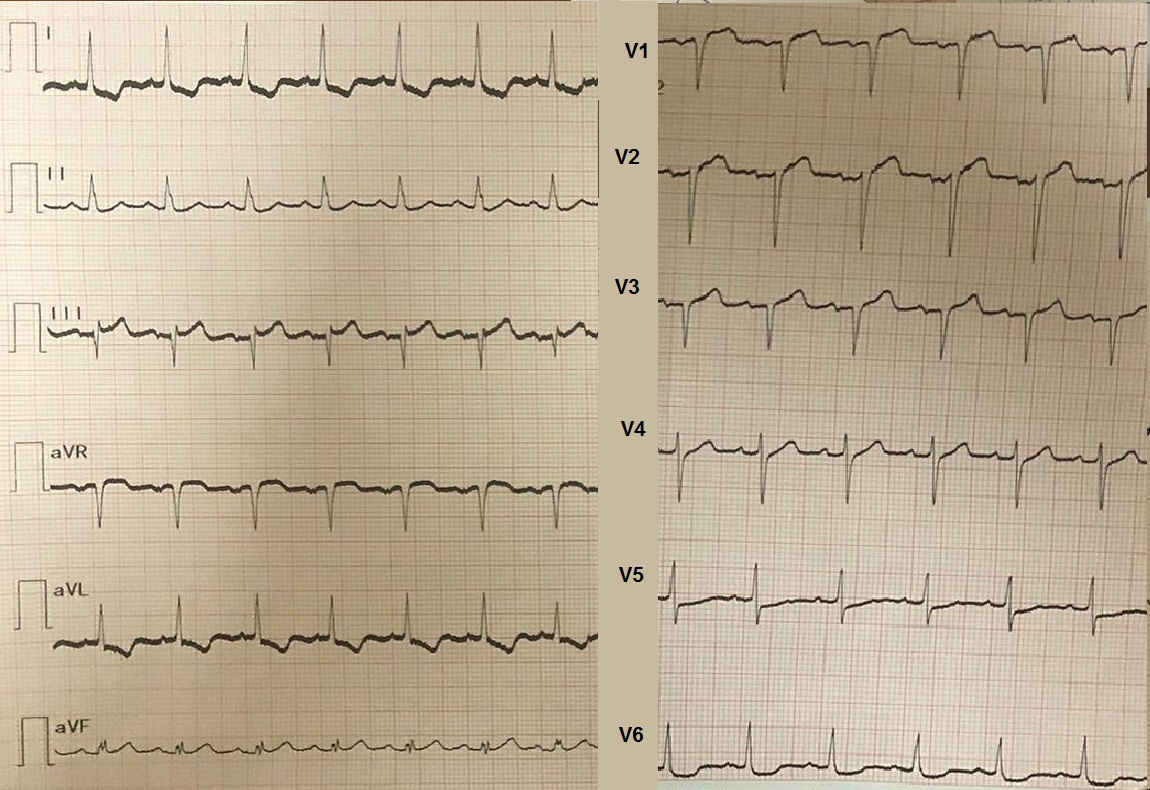
A 54-year-old male patient with renal transplant(15 years ago) had complained persistent rest angina for2 days. These symptomsmissed to be associated with an acute myocardial infarction. His ECG showed STelevation from V1 to V3 and ST depression in D1,aVL, V1 and V6. He was anxiousand agitated. His BP was 110/70 mm Hg. Heartrate was 118 bpm and respiratoryrate was 26 per minute. A subacute anterior infarction with post MI anginahad been suspected
Relevant Test Results Prior to Catheterization
Aspartate transaminase (105 U/L), Lactate dehydrogenase (290 U/L) andtroponin (6536 pg/ml) levels werehigh to indicate a myocardial injury. At the same time, the patient hadincreased blood urea (155.5 mg/dL) and creatinine (3.75 mg/dL) level, which decreased to 101 mg/dL and 2.24 mg/dL respectively after the procedure. Uric acid (12.5 mg/dL), glucose (134 mg/dL), CRP (94.95 mg/dL) and leukocyte (12.490) were also elevated.
 Video 1. Right coronary artery.avi
Video 1. Right coronary artery.avi
Video 2. Left coronary system.avi
Video 3. LAD after predilataion.avi
Relevant Catheterization Findings
Interventional Management
Procedural Step
As far as we know, only few stenting techniques have been defined in the treatment of Medina 0,1,0 or 0,1,1 left main stenosis. LM-to-LAD crossover stenting is a good technique to treat LAD ostial stenosis, but many operators still want to put a stent just limited to LAD. In our technique, we impanted a 3.0x20 mm DES in the LAD ostium with 1-2 mm protrusion into the LM after predilatation and performed final kissing ballooning with a 2.0x20 mm balloon which is already parked in the ramus branch. Precise stent placement in the LAD ostium is technically challenging. Excessive protrusion of the stent into LM might result in stent deformation and compromisation of future interventions. On the other hand, geographic miss leaving a portion of the lesion uncovered is related to edge dissection, restenosis, stent thrombosis. Szabo and Afzal's techniques are focal ostial stenting strategies which are developed to minimize incomplete lesion coverage (geographic miss) in the ostium. As expected in all techniques, jailing or loss of side branch (LCX) due to plaque shift are inevitable in some circumtances . In Stent-Λ-Balloon Technique, a prompt intervention in such complications could be possible with a parked safety balloon, which is first used as a marker for stent positioning. Parked safety balloon could also be inflated simultaneously to prevent plaque shift or after stent implantation to improve carina and crush unnecessary stent protruding into left main over LCX.
Video 7. Final angiography.avi
Case Summary
The name Stent-Λ-Balloon Technique is inspired by Λ-kissing in LM with minimal overlap of stent balloon and safety balloon.Similar to Afzal's technique, a balloon has been parked LM-to-LCXas a marker. After stent implantation, kissing balloon is usually appliedespecially if there is a narrow angle between LAD and LCX. Parked safetyballoon could be inflated together with stent for a prophylaxis purpose if possibility of plaque shift is too high. In conclusion, Stent-Λ-Balloon Technique might be used in the treatmentof LAD ostial stenosis which allows precise positioning of a stent, prevents/treatspossible plaque shifting and crushes unnecessary stent over LCX ostium.