
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-022
Left Main Artery Acute Myocardial Infarction With Cardiogenic Shock in a Patient With Type a Aortic Dissection Post Aortic Graft and Aortic Valve Replacement
By Chin-Feng Tsai, Yao-Tsung Chuang
Presenter
Yao-Tsung Chuang
Authors
Chin-Feng Tsai1, Yao-Tsung Chuang1
Affiliation
Chung Shan Medical University Hospital, Taiwan1,
View Study Report
TCTAP C-022
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Left Main Artery Acute Myocardial Infarction With Cardiogenic Shock in a Patient With Type a Aortic Dissection Post Aortic Graft and Aortic Valve Replacement
Chin-Feng Tsai1, Yao-Tsung Chuang1
Chung Shan Medical University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. Cho
Relevant Clinical History and Physical Exam
Relevant clinical history
Relevant Test Results Prior to Catheterization
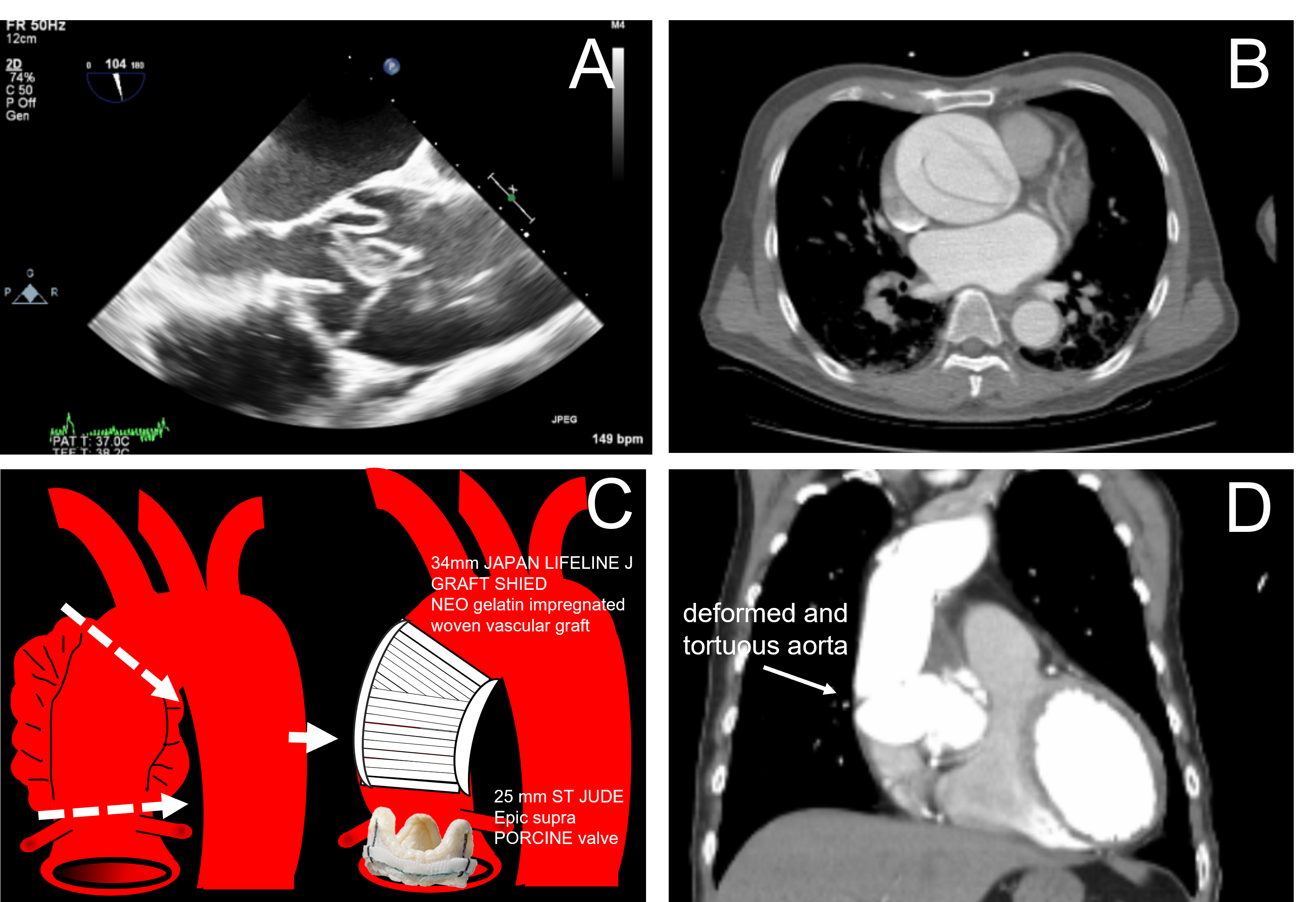
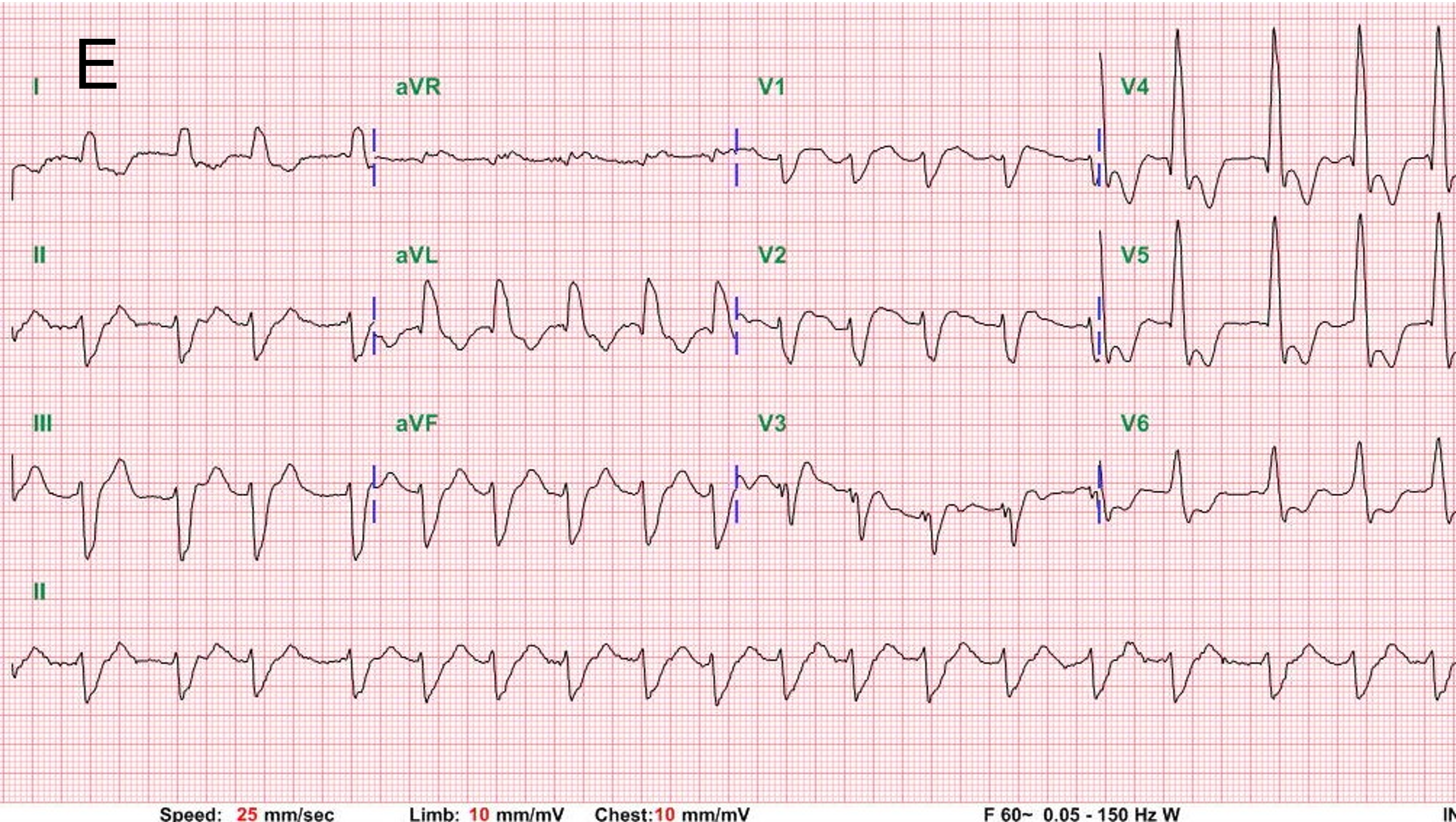
baseline EKG revealed atrial fibrillation with rapid ventricular response ;Chest radiography revealed cardiomegaly and no pulmonary edema,chest computed tomography (CT) revealed no recurrent aortic dissection and deformed aorta (figure D);EKG on episode day revealed AVR ST elevation with diffuse ST depression (figure E), new onset left bundle branch block
Relevant Catheterization Findings
coronary artery angiography revealed left main artery ostium 99% stenosis(figure F); difficult to engage to right coronary artery
Interventional Management
Procedural Step
The left coronary artery was engaged by a JL 4.5; SH guide catheter; then a field Fc wire was passed through the left main lesion, and the left main lesion was direct stenting with a 4.5 x 12 mm drug-eluting stent (Abbott, Xience); post dilatation was done by a 4.5x 8 mm NC balloon with 18 atms .(figure G) There was no residual stenosis. No IVUS evaluation because of cardiogenic shock. We did not perform right coronary angiography because of difficult engaging the right coronary artery. after left main artery stening , shock status improved .

Case Summary
Iatrogenic coronary ostial stenosis (ICOS) may involve one or both coronary ostia , LM stenosis is most frequent.It`s Incidence is 0.5-5%.It may induced acute coronary syndrome , ventricular arrhythmia or heart failure. it often occurred within 6 months of cardiac surgery. PCI appears to be the best revascularization option .About Antithrombotic agents use , reduced-dose regimens ,Short-term DAPT, Early P2Y12 inhibitors monotherapy and Phenotype- or genotype-guided individualization may be the optimal strategies for a east Asian