Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200411_003
| CORONARY - Complications | |
| The Houdini Case- Extirpation Of Stucked Ostial LCx Stent In The Struts Of Previous Implanted Ostial LAD Stent, Ending Up With Two Extirpated Stents | |
| Oktaj Maksudov1, Farhat Fouladvand2 | |
| Bulgarian Cardiac Institute, Bulgaria1, Clinica San Carlo, Italy2, | |
|
[Clinical Information]
- Patient initials or identifier number:
C.M.
-Relevant clinical history and physical exam:
Male,72y.o, retired, was reffered to our hospital as Stabile ungina III CCS. Thepatient got positive family anamnesis for CAD with previous coronaryprocedures/ PCI/Stenting to mid.RCA and distal RCA due to inferior STEMI/2018/and PCI/Stenting to ostial LAD/also 2018, 1moth before the presenthospitalization. From comorbidities the patient got diabetes/on insulin/. Fromphysical exam with stabile cardiopulmonary status.
-Relevant test results prior to catheterization:
From non invasive methods:
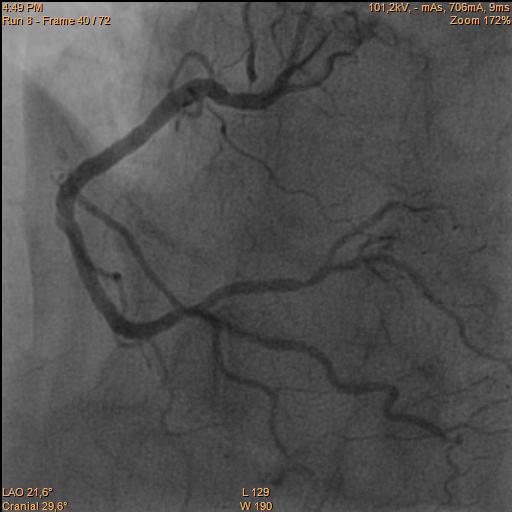
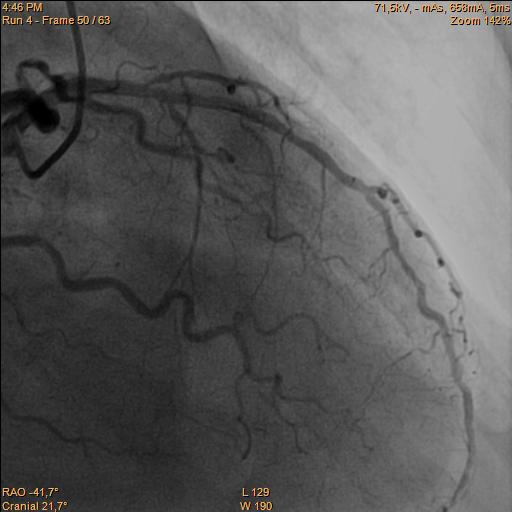
- Relevant catheterization findings:
Angyo was done through right radial artery/6F indroducer.
   |
|
|
[Interventional Management]
- Procedural step:
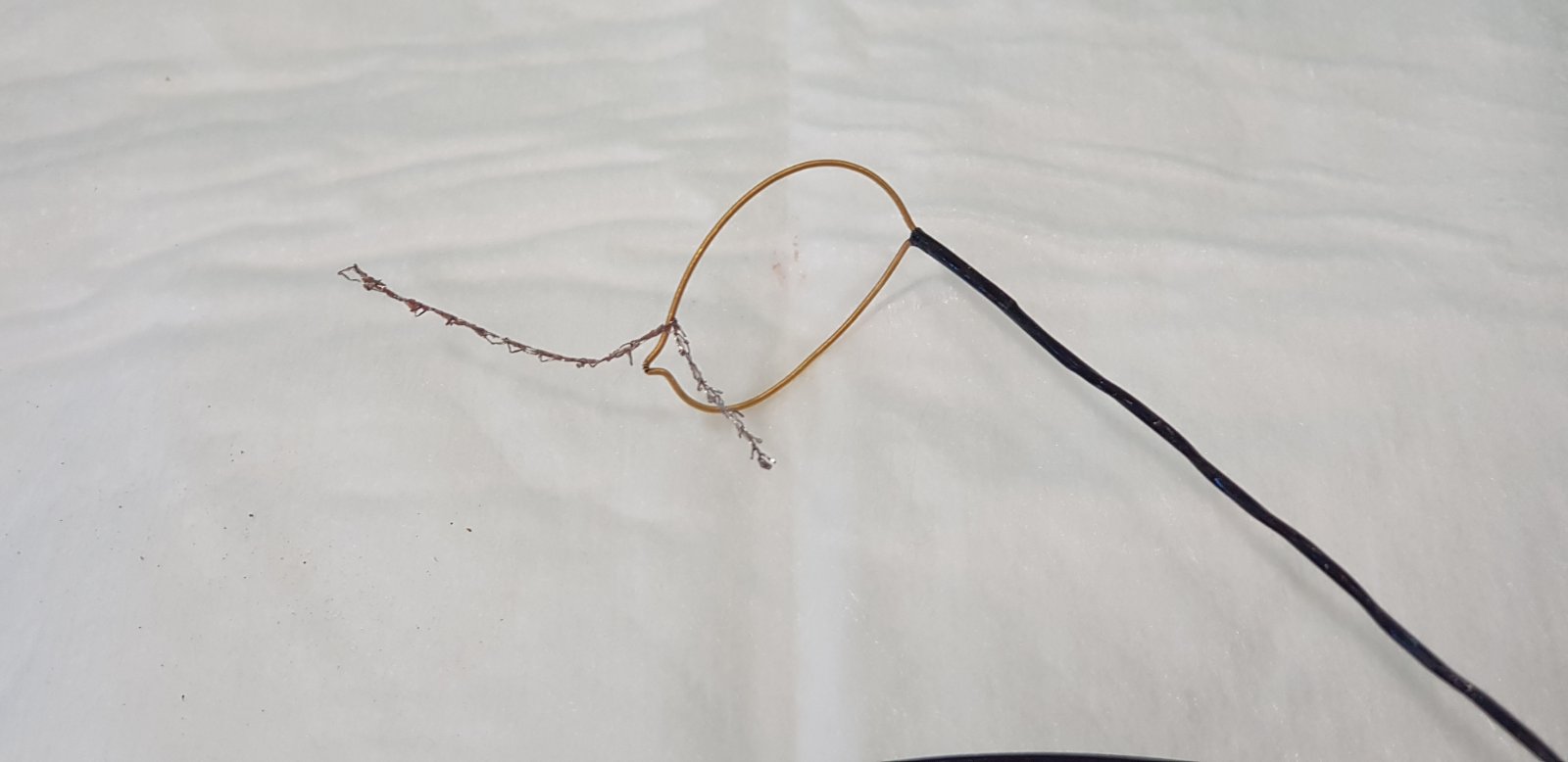
PCI/GC EBU 3.5/6F, GW-BMW placed in LCx. Wedid pre-dilatation with baloon 2.0/30mm. After that we tried to implant DES2,25/24mm but the stent could't pass trough LM. We tаке out the stent, but onlybaloon was on the shaft. So what happened was that we passed with GW trough the strut of the ostial placed stent inLAD, that was implanded previous month and the stent we've tried to implant indLCx falled off the baloon and was stucked in the strut of ostial LAD stenttowards LM . We’ve got 3 plans for resolving the situation: PLAN A -With smallbaloon trying to push the stent down, away from LM, but that was withoutsuccess, PLAN B -Triyng to crush the stent and we took Guideliner ,trying tosecure support for bigger ballon to pass and crush the stent towards LM ,butalso this was failed attempt. And bailout was PLAN C- Stent retrieval, so wetook loop snare and managed to catch the stent. We were satisfied that the jobwas finished, but we've managed only to extract the proximal part of the stent.The rest of the stent was still there, stucked in the ostium od LAD. So we takethe snare again and this time we managedto extract the stent, but when we took out the stent we're very surprised thatin fact with the stucked LCx stent we’ve extirpated the ostial LAD stent. Intaking out a part of the stent fell out in front of radial sheath. We continuedtrough right femoral artery , did aortography at first/the aorta was ok/, then IVUS/LM/LCxand PCI/LCx and LAD in same act.
 - Case Summary:
Conclusions
|
|