Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200407_002
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| PTA for the ostial lesion of the superficial femoral artery via an ipsilateral antegrade approach, | |
| Jino Park1, Dong-Kie Kim2, Yeo Jeong Song3, Seunghwan Kim1 | |
| Haeundae Paik Hospital, Korea (Republic of)1, Inje University Haeundae Paik Hospital, Korea (Republic of)2, Inje University Busan Paik Hospital, Korea (Republic of)3, | |
|
[Clinical Information]
- Patient initials or identifier number:
NDS
-Relevant clinical history and physical exam:
The patient was an 80-years-old man with intermittent claudication (150m) of the right leg. He had multiple comorbidities but didn’t have any risk factors for atherosclerosis like diabetes, hypertension, or smoking. The pulsation of the right dorsalis pedis was not palpable.
-Relevant test results prior to catheterization:
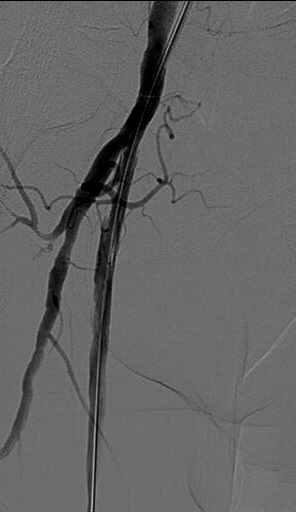
CT angiography revealed a long segmental occlusion of the Rt. SFA and a constituted popliteal artery (Figure). Ankle-Brachial Index (ABI) finding was right 0.58/left 0.97.
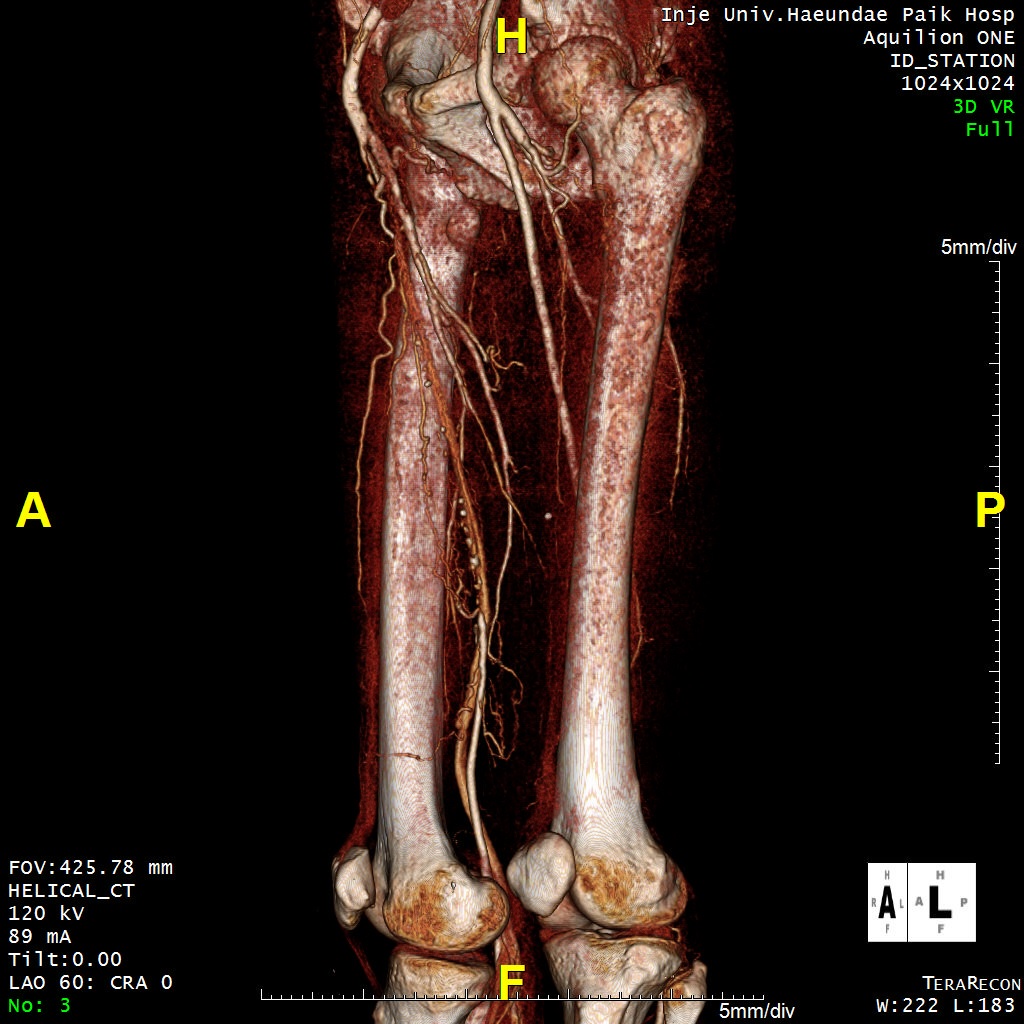 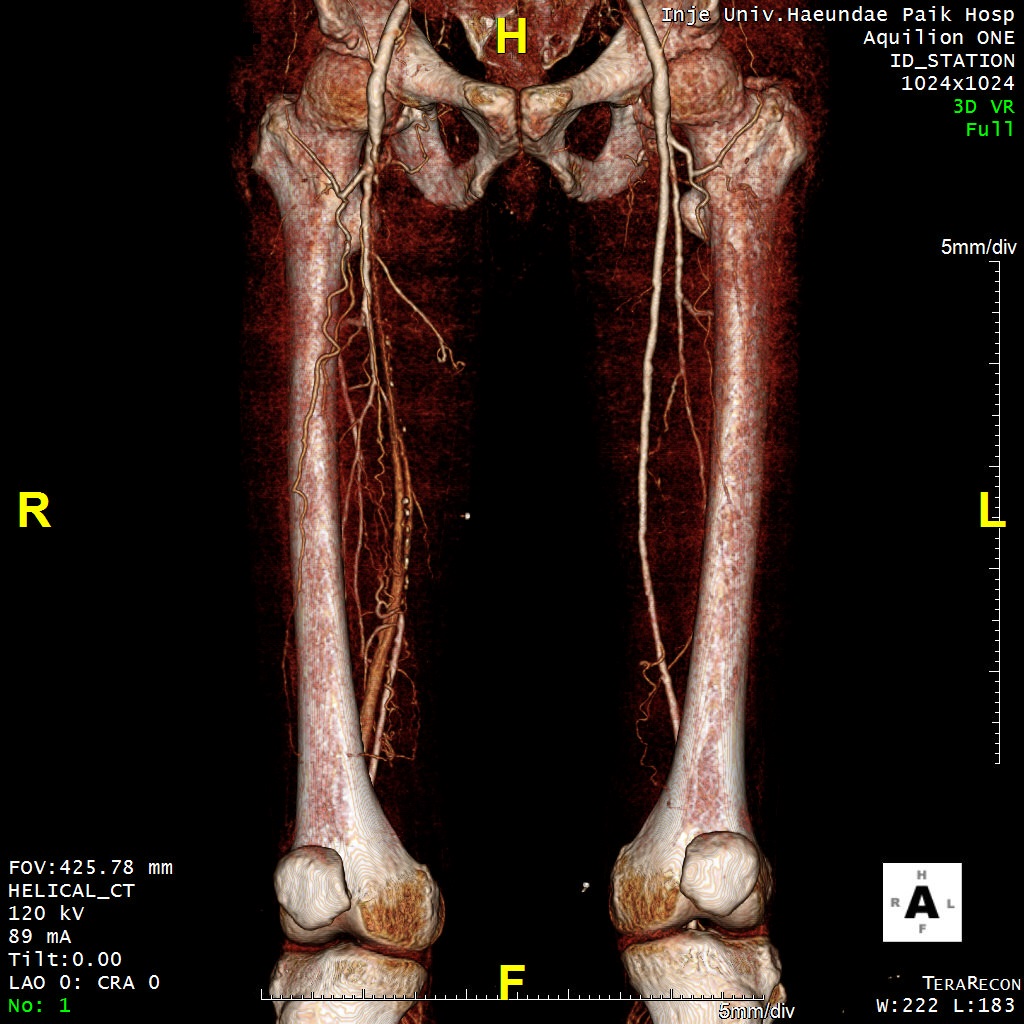 - Relevant catheterization findings:
The Rt. SFA showed total occlusion from ostium to distal SFA (Figure). And the total occlusion of right ATA and PTA was also shown.
 |
|
|
[Interventional Management]
- Procedural step:
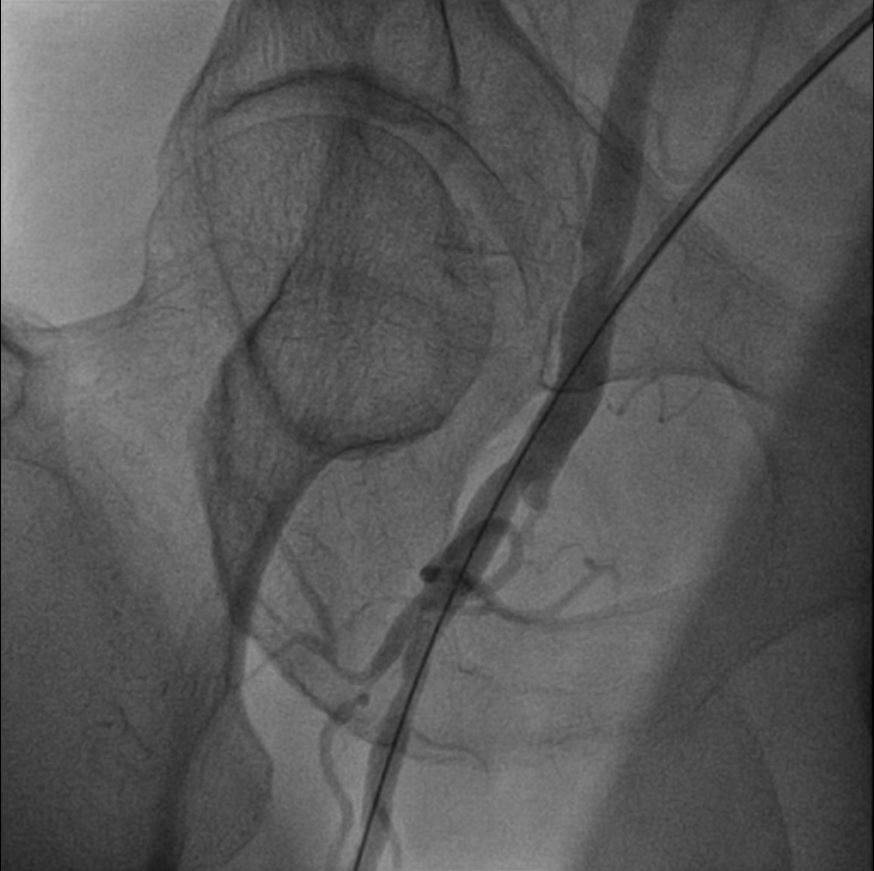
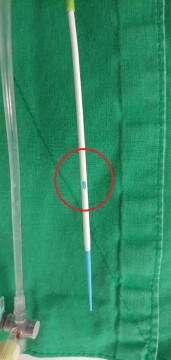
Due to the problem of femoral artery puncture and sheath insertion due to the location of the lesion, total occlusion from the ostium of the Rt. SFA, the ipsilateral anterograde approach was limited. Therefore, it was necessary to proceed to the contralateral approach. In this case, there is a disadvantage that supporting is not good compared to the ipsilateral approach. To overcome this, we made a hole on the sheath surface 3 cm proximal from the sheath tip (figure). And then, we punctured the Rt. CFA and inserted the sheath into the DFA. With the sheath mounted on the DFA, the 0.14 Command wire was wired to pass through the artificially created side hole entrance, and it approached the ostial lesion of the SFA and crossed the lesion relatively easily (video).The sheath in the DFA was repositioned to the SFA while the wire was mounted on the distal of the SFA. And intraluminal wiring succeeded under supporting using CXi microcatheter. Then, POBA was performed on an SFA lesion with a mustang 4.0x120 mm balloon. The InPact Admiral 5.0x150 mm DCB was applied to the mid-SFA, and the InPact Admiral 6.0x150 mm DCB was applied to the proximal SFA. There was a minor dissection, but no flow limitation was observed (figure). The procedure was finished successfully without any complications. After the PTA, the patient’s claudication was relieved, and his ABI finding of the right ankle was improved from 0.58 to 0.97.
  - Case Summary:
If there is a lesion in the ostium of SFA, due to the problem of femoral puncture and sheath insertion, a contralateral approach is inevitable. In this case, weak support becomes a problem when compared to the ipsilateral approach. In the PTA for the ostial lesion of SFA, the ipsilateral antegrade approach using the side hole of the sheath mounted on the DFA may be a practical option.
|
|