Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191203_001
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Unpredictable End | |
| David Baghdasaryan1 | |
| Nork-Marash Medical Center, Armenia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
AA
-Relevant clinical history and physical exam:
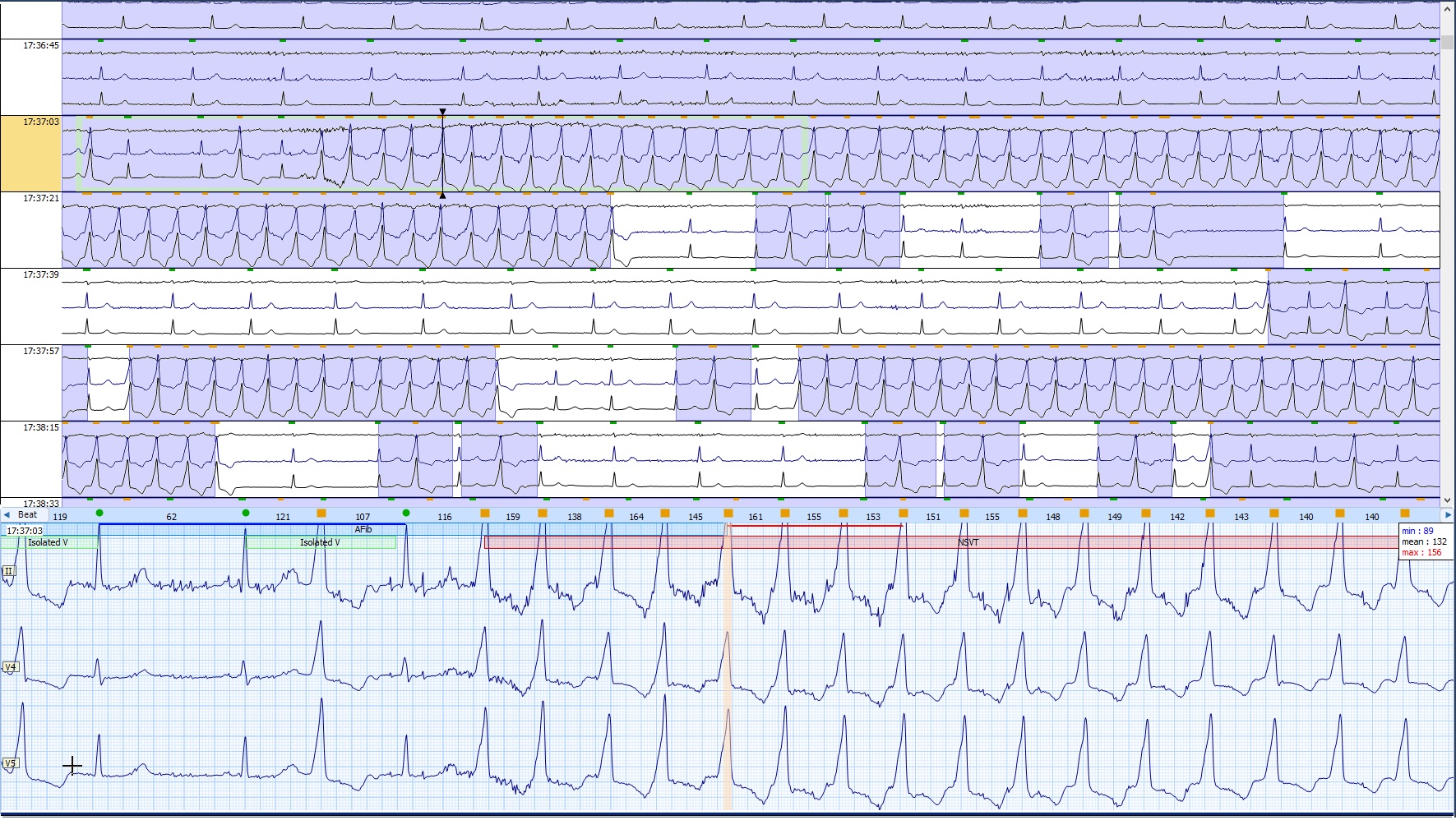
A 32-year-old female underwent a planned electrophysiological procedure, followed by ablation, in connection with the diagnosis of violation of the heart rate, particular frequent lonely monomorphic premature ventricular extrasystoles (PVCs) and nonsustained ventricular tachycardia (NSVT). Objective data and biochemical blood tests were normal. She does not have concomitant diseases and has no bad habits. Does not take any medicine. Anamnesis is not burdened with cardiovascular diseases.
  -Relevant test results prior to catheterization:
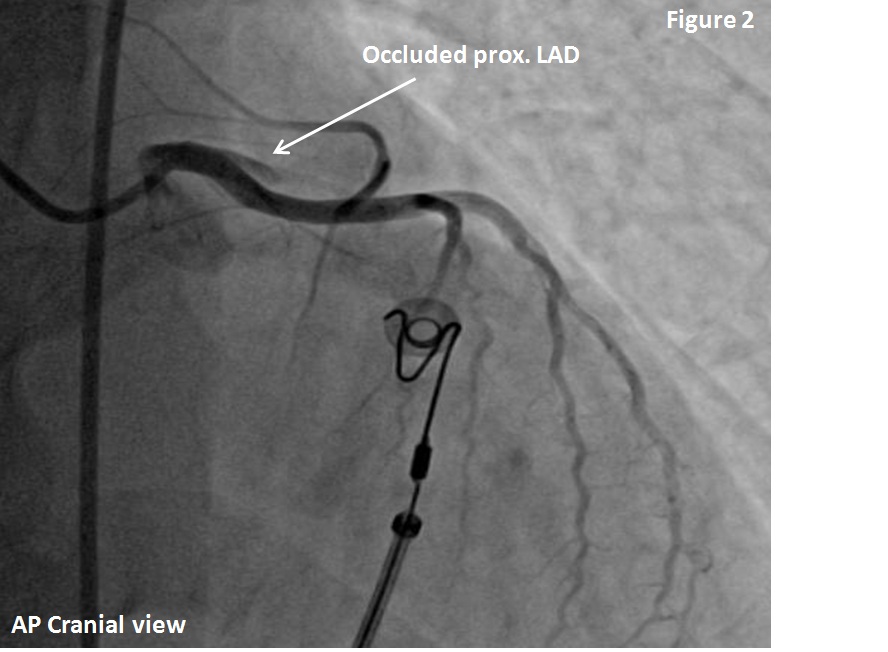
Ablation was performed through the right femoral arterial access (7Fr introducer), by an irrigated radio-frequency catheter (Cath) under the conditions 30W and 55°C and also with 4mm non-irrigated Cath in the region of LVOT, below left coronary cusp, where did the activity come from.
 - Relevant catheterization findings:
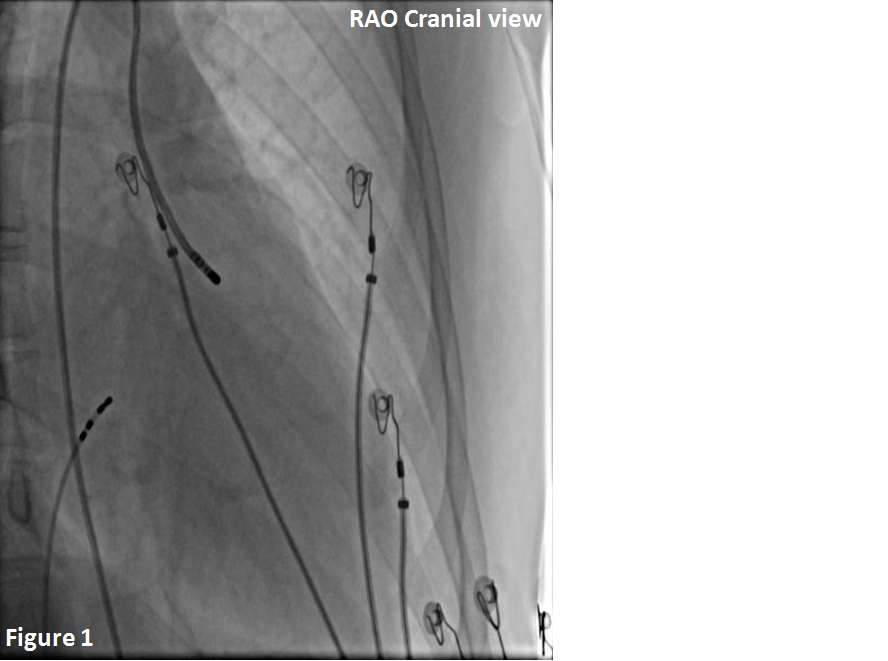
During ablation, the patient began to complain of severe chest pains and on ECG was recorded ST elevation in V1-V6 leads. Urgently, CAG was performed and signs of spontaneous coronary artery dissection (SCAD) of the proximal LAD with complete occlusion were revealed.
 |
|
|
[Interventional Management]
- Procedural step:
It was urgently recanalized LAD. Tools was 6 Fr XB 3.5 Guide Catheter and 2 Runthrough Floppy Guide wires. After recanalization and balloon predilatation with 2.0 x 15 mm semi-compliant balloon, the distal part of the artery was not visible. A manual thromboaspiration was also performed and a contrast was selectively injected into the distal part of the artery by the aforementioned catheter, after which it was clear that the hydrophilic guide wire in the large septal branch and the LAD was already visible retrograde. After multiple and not easy attempts, the guide wire was successfully carried to the distal part of the LAD. In dynamics the dissection also retrograde spread to left main (LM) and in the mid part of left circumflex artery (LCx). At first there was a stented LCx with 3.0 x 30 mm drug eluting stent (DES), and after prox LM to the LAD with 4.0 x 30 mm DES and then the mid LAD with 3.0 x 23 mm DES, as the dissection spread to this part. In the end, final kissing balloon postdilatation (FKB) was done with 4.0 x 15 mm (LM - LAD) and 3.0 x 15 mm non-compliant (NC) balloons, respectively.
- Case Summary:
Not a frequent, but life-threatening complication during ablation, after which the flap closed the lumen of the LAD. Complicated by the fact that the dissection spread to the LM and LCx. Due to the rapid intervention, the coronary arteries were stent with 3 DES and the patient's condition stabilized. The result was satisfactory and the patient, after intervention on the 5th day, was discharged from the hospital without complications.
|
|