Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191117_004
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Non-Invasive | |
| Local Intracoronary Fibrinolytic Alteplase in Acute Anterior Myocardial Infarction Patient (Single-Photon Emission Computerized Tomography-SPECT Result) | |
| Furqan Arief1, Dika Ashrinda2, Muhammad Desfrianda Pane2, Hilfan Ade Putra Lubis1, Zulfikri Mukhtar1, Ali Nafiah Nasution2, Harris Hasan2 | |
| Adam Malik General Hospital, Indonesia1, University of Sumatera Utara, Indonesia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
AS
-Relevant clinical history and physical exam:
A 27-year-old man presented with typical cardiac chest pain of acute coronary syndrome since 8 hours before hospital admission. Risk factor is smoking.
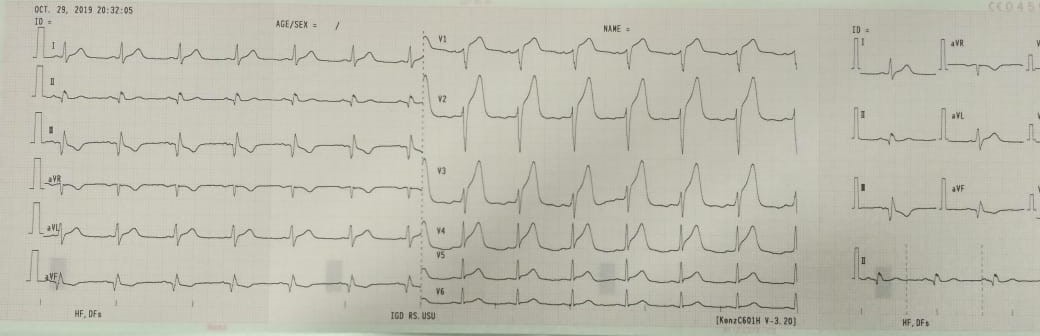
BP: 110/70 mmHg, HR: 70x/i RR: 22x/iHeart: normal heart sound -Relevant test results prior to catheterization:
ECG: Sinus Rhythm, ST-Elevation at V1-V5Cardiac Enzyme: Troponin T : 1048 ng/L, CKMB : 40.46 ng/mL.
  - Relevant catheterization findings:
Coronary angiography showed total occlusion at mid portion Left Anterior Descending (LAD) Artery, TIMI flow 0. Normal Left Circumflex (LCx) Artery and Right Coronary Artery (RCA).
Steps of procedural angioplasty. |
|
|
[Interventional Management]
- Procedural step:
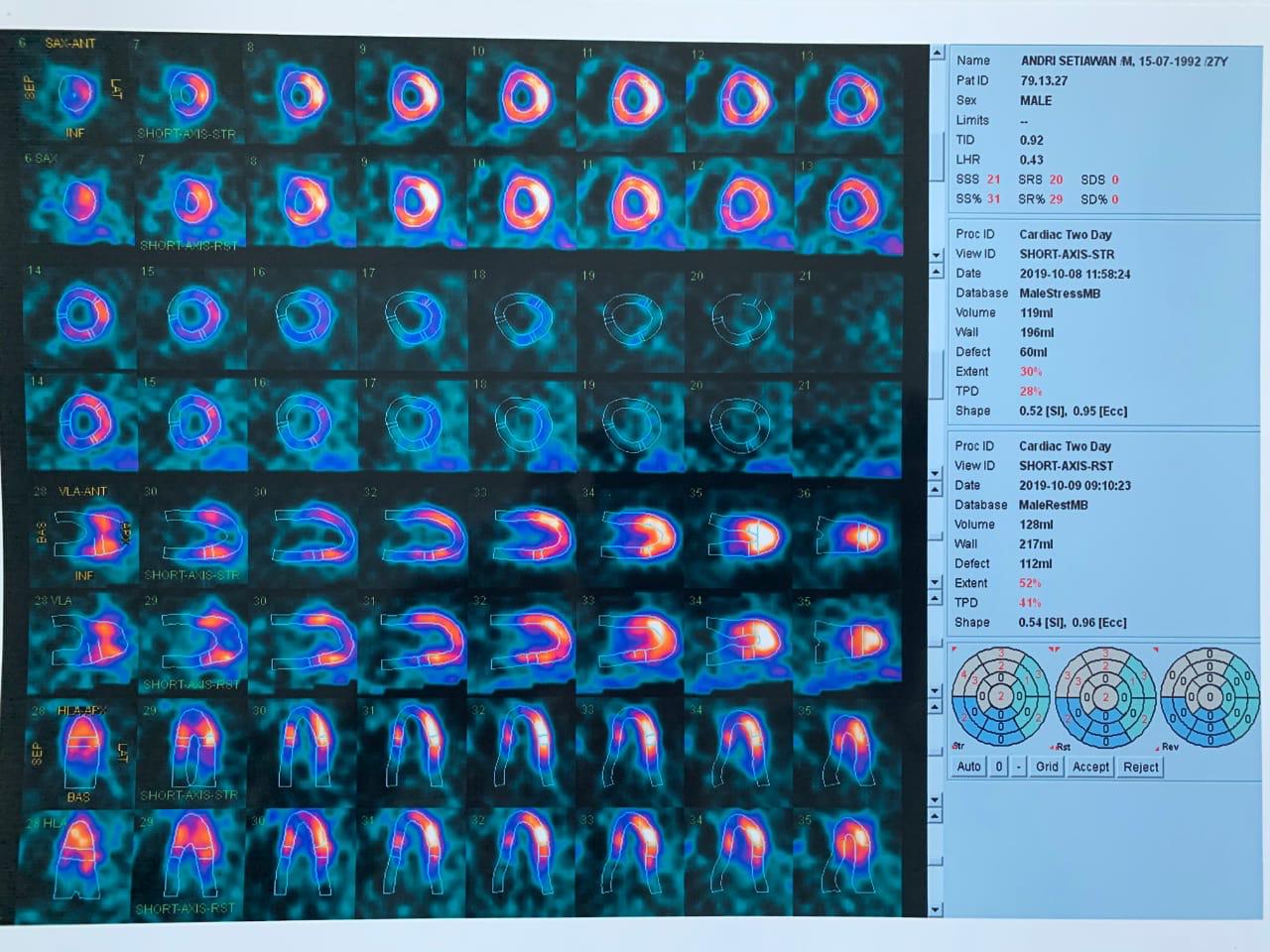
The using of XB guiding catheter 3, 6F, the guide wire from left main artery was directly into Left Anterior Descending and followed by balloon (1.5 x 15 mm) inflation 14 atm, 10 seconds, continued manual injected Alteplase3 mg in 10 mL saline in 3 minutes. The procedure was continued with placement and deployment Stent (DES), 3.0 x 24 mm at stenotic mid of LAD. After stent deployment NTG 200 µg was added. Two weeks later, SPECT examination showed normal blood flow in the apical septal and mid-apical anterior wall, and fixed defect in basal apical and basal anterior septal.
- Case Summary:
A 27-year-old man presented with typical cardiac chest pain of acute coronary syndrome since 8 hours before hospital admission. Coronary angiography showed total occlusion at midportion Left Anterior Descending (LAD) Artery, TIMI flow 0. Normal Left Circumflex (LCx) Artery and Right Coronary Artery (RCA). He successfully underwent primary angioplasty with 1 stentimplantation. Two weeks later, SPECT examination showed normal blood flow in the apical septal and mid-apical anterior wall, and fixed defect in basal apical and basal anterior septal. Echocardiography found LVEF54 % (Simpsons).
|
|