Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_037
| CORONARY - Chronic Total Occlusion | |
| Ipsilateral Reverse Processing of LAD-CTO | |
| Li Chenggang1 | |
| Heart center of Xuzhou Third People's Hospital, China1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. WU
-Relevant clinical history and physical exam:
Age: 78 years old Sex: Male
Chief compliant: Sustained chest pain for eight hours Risk factor: Hyperlipidemia and smoking Past history: Cerebral infarction and irregular use of aspirin and statins elevation Coronary atherosclerotic heart disease Acute inferior ST-segment elevation myocardial infarction Killip Class I Cerebral infarction -Relevant test results prior to catheterization:
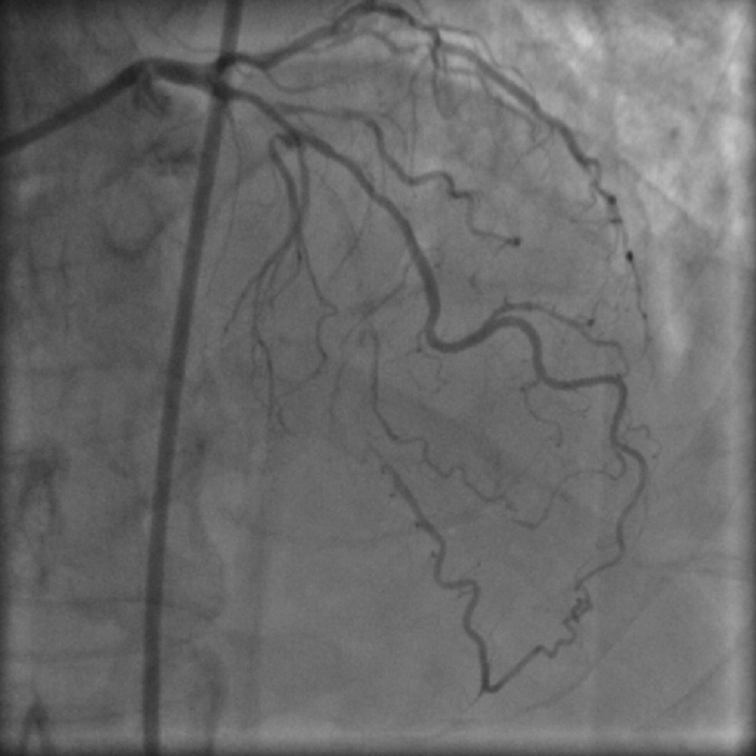
- Relevant catheterization findings:
mLAD-CTO ipsilateral collateral circulation to pLADmLCX 80% stenosisdRCA 90% stenosis mRCA 95% stenosis with thrombus
   |
|
|
[Interventional Management]
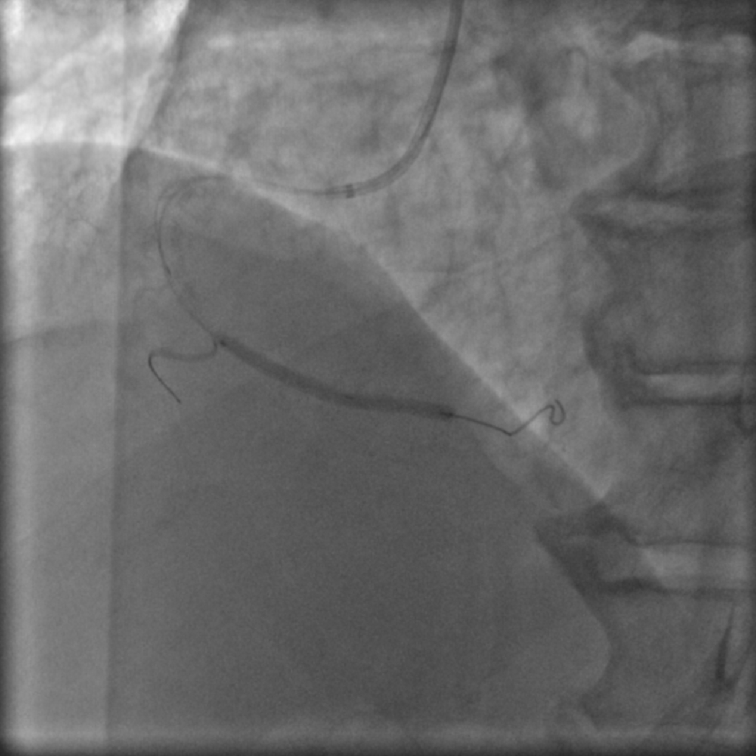
- Procedural step:
The patient with AMI was admitted to the hospital, and after the IRA
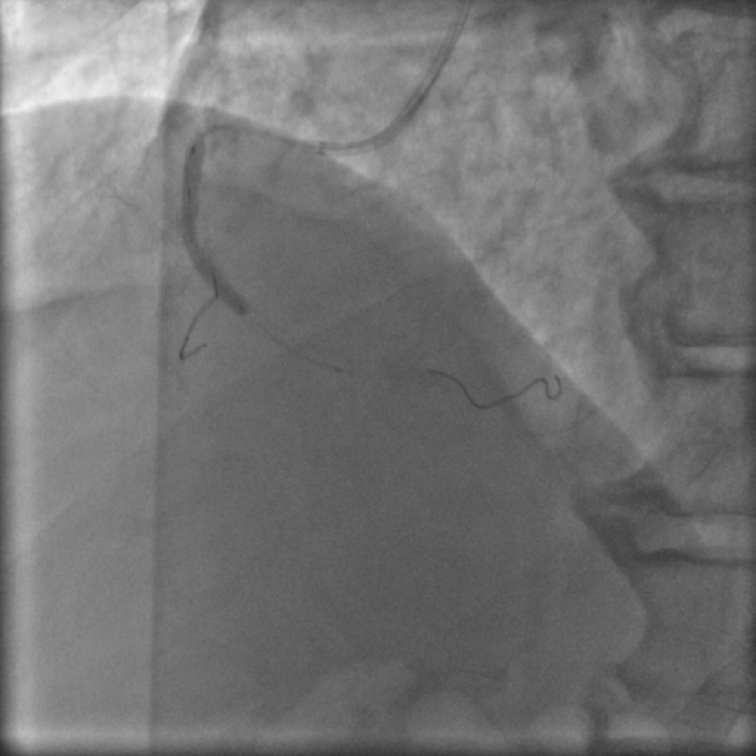
was confirmed by the emergency PCI, the stent was implanted. The LAD-CTO was treated electively. J-CTO score was 3, IVUS failed to indicate the lesion entrance, so the first choice was reverse interventional therapy. Two epicardial collateral branches, one is thick and twisted, the other is thin and straight, which are tried carefully repeatedly and finally passed through the thin collateral branch. Considering the serious calcification, the high penetration guidewire is the first choice for reverse attack, and finally the guidewire is upgraded to pilot 200 to reverse break through the distal fiber cap. One year later,we review coronary angiography to confirm that LAD was patency. - Case Summary:
Considering the difficulty of Finecross microcatheter passing through the occluded lesions, the modified rendezvous technique was used to complete the final antegrade. IVUS confirmed that the guide wire was located in the true lumen, and then balloon expansion and stent implantation were completed successfully. Review after one year, the stent is unobstructed, and the patient finally gains clinic benefits. |
|