Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_031
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Two Lives at Stake | |
| Tanveer Iqbal Penwala1, Afrah Yousif Haroon1, Rosli Mohd Ali2, Al Fazir Omar1 | |
| National Heart Institute, Malaysia1, Cardiac Vascular Sentral Kuala Lumpur, Malaysia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
NM
-Relevant clinical history and physical exam:
25-year-old pregnant lady at 12 weeks of pregnancy presented with chest pain and complaining of almost daily angina. She was also a known case of hypertension and familial hyperlipidemia. She was diagnosed with severe ostial LMS disease and severe RCA disease one year ago. Her echocardiography showed severe aortic stenosis. She was planned for CABG and AVR but she defaulted follow-up. After multidisciplinary discussion decision was made for PCI first then aortic valve replacement later.
   -Relevant test results prior to catheterization:
Creatinine 39, Hemoglobin 11.7, Platelet 225 Total cholesterol 17.7LDL 15.3
- Relevant catheterization findings:
Severe LMS disease and severe ostial RCA disease
  |
|
|
[Interventional Management]
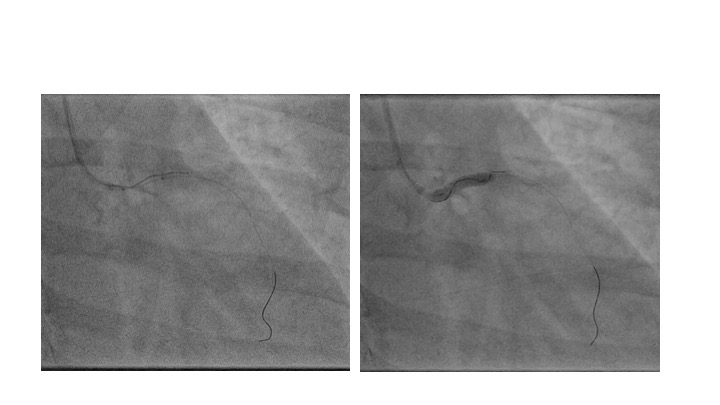
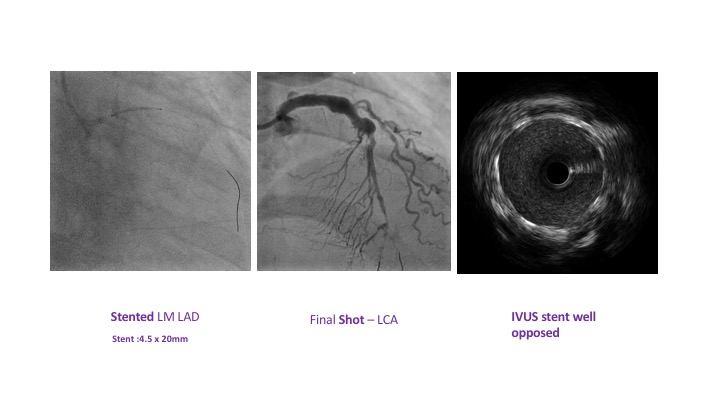
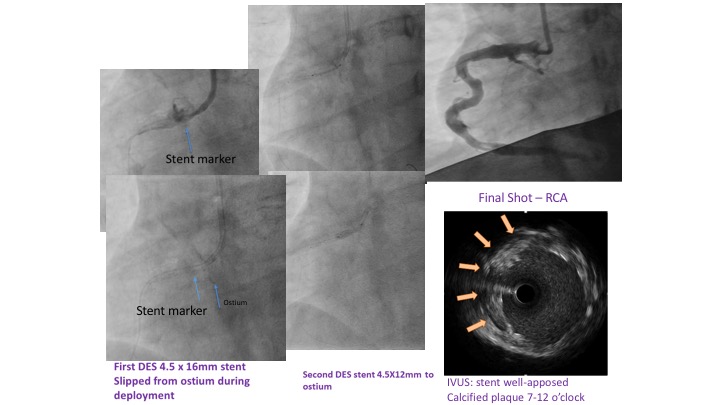
- Procedural step:
Right radial approach and 6F radial sheath used . RADPAD protection applied. Due to the huge chunk of calcium in aortic root, there was difficulty engaging the left system. EBU 3.0/6F was used followed by SAL1/6F then AR2.0/6F then JR3.5/6FThe LMS was short and the vessel ectatic so had to wire the LMS-LAD from outside using run through floppy wire. Predilated LMS done with Sapphire 2.0 x 15mm at 16 atmospheres. Then predilated further the LMS with Sapphire 4.0 x 15mm at 16 atmospheres. Reattempt wiring Lcx with crusade microcatheter. Changed to Fielder XT- Pilot 50. Still unable to wire the LCx. Decided to proceed LMS- LAD stenting. Stented LMS-LAD with CRE8 4.5 x 20mm at 18 atmospheres. IVUS showed ostial LMS stent well apposed. Next, proceed with PCI to RCA. Rewired RCA with run through floppy wire. Predilated ostium RCA with Sapphire II 2.0 x 15mm at 16 atmospheres then Sapphire II 3.0 x 15mm at 20 atmosphere then Sapphire NC 4.5 x 15mm at 28 atmospheres. Stented with CRE 8 4.5 x 16mm at 10 atmosphere. Noted stent slipped forward when deploying missing the ostium. Stented ostium with CRE 8 4.5 x 12mm at 20 atmospheres. IVUS showed stent well apposed.
   - Case Summary:
The procedure was uneventful. Radiation to the fetus was reduced by using RADPAD protection. Baby was safely delivered 6 months later in our centre via elective Caesarean section and the patient undergone bilateral tubal ligation. She continued to be under our centre follow-up. Both mother and baby are well. This case illustrates a successful treatment of coronary artery disease in pregnancy in which PCI could not be delayed due to acute cardiac event and persistent symptoms.
|
|