Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_017
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Multivessel Disease in STEMI: Should We Stick to “Culprit Only” Strategy? | |
| Deri Arara1, Muhammad Fadil2 | |
| M. Djamil Hospital, Indonesia1, Binawaluya Heart Hospital, Indonesia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. A, 66 years old
-Relevant clinical history and physical exam:
A 66 years old male patient with cardiovascular risk factors (smoker, dyslipidemia, age) was admitted on the ER with a diagnosis of STEMI anterior extensive. The general examination reveals a stable general condition, normal rhythmic heartbeats without any heart murmurs and without rales. We performed PPCI at osteal-mid LAD. In the 3rd day of hospitalization, patient was planned to be discharged but suddenly he got seizure and the ECG showed VT. Then were performed PCI.
-Relevant test results prior to catheterization:
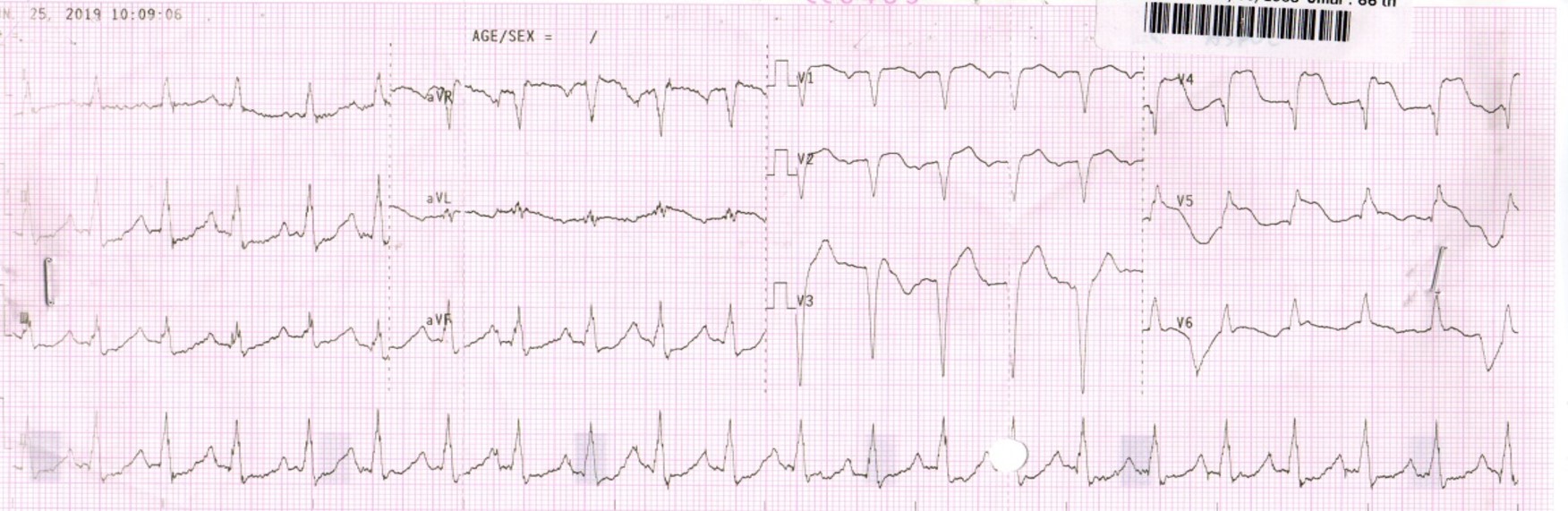
The electrocardiogram performed on ER shows ST elevation 2-5 mm in leads V1-V6, I, aVL with ST depression II, III, aVF and the positive troponin I value. The patient was rushed to the cath lab for primary PCI.
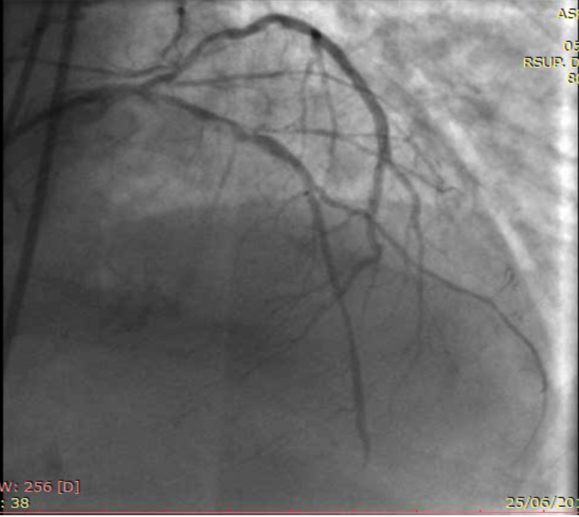
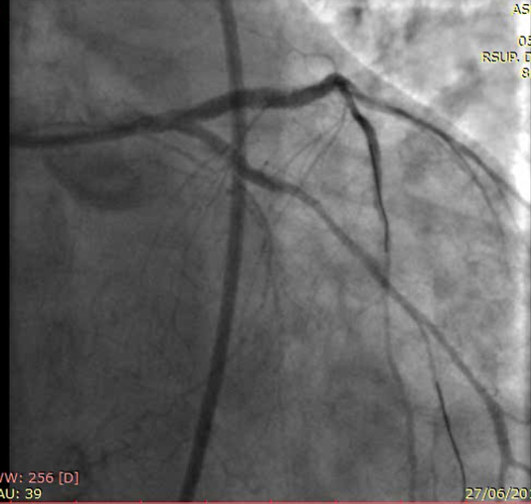
 - Relevant catheterization findings:
The CAG showed subtotal occlusion at proximal LAD with thrombus burden grade III, CTO at distal LCX and significant stenosis at LM (60-70%) and mid-distal RCA. We performed PPCI at osteal-mid LAD with TIMI flow 3 and MBG 3 as a result. In the 3rd day of hospitalization we performed re-PCI with culotte technique to overcome the bifurcation lesion. It took two drug-eluting stents implanted into osteal LM- proximal LAD and distal LM-proximal LCX with a satisfactory result.
|
|
|
[Interventional Management]
- Procedural step:
At the first procedure, we performed CAG using 6fr BL guiding catheter. we advance soft wire using ASAHI SION blue to the LAD. We performed multiple inflate balloon 2.5x15 mm at LAD. After that we decide to performe PCI using DES stent 2.75 x 26 mm and 2.75x16 mm at proximal-mid LAD.At the re-PCI we performed LCA graft using 6Fr SBS guiding catheter. We advance the lesion using ASAHI SION blue wire to LCX and also LAD. We performed multiple balloon inflation at LM-LAD and LM-LCX using semi compliance balloon 2.75x15 mm with 9-14 atm pressure. After that we implanted DES 2.75x26 mm at distal LM-Proximal LCX with 9 atm pressure. Then we switch the wire form LAD to LCX and LCX to LAD. After that we inflated the 3.0x15 mm semi compliance balloon to osteal LM-proximal LAD 10-12 atm for 10 seconds. After that we implanted DES 3.0x18 mm to osteal LM-proximal LAD with 10 atm pressure twice. After that we switch the wire LAD and LCX again. Then we put stent balloon 3.0x18 mm to distal LM-proximal LAD and non-compliance balloon 2.75x12 mm to distal LM-proximal LCX and we performed kissing balloon 4-5 atm.
   - Case Summary:
Among patients with STEMI and multivessel coronary artery disease, we must consider to performe the non-IRA revascularization during the hospitalization to reduce the major adverse cardiovascular event.
|
|