Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_012
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| LM Bifurcation via Radial Approach Using Sweep Balloon to Assist LCx Wiring and Balloon Anchoring Technique for Stent Delivery | |
| Panu Dumrongkitchaiporn1 | |
| Ramathibodi Hospital, Thailand1, | |
|
[Clinical Information]
- Patient initials or identifier number:
CP
-Relevant clinical history and physical exam:
A 85-year-old female admitted for elective coronary angiogram due to progressive dyspnea on exertion and positive exercise stress test. She had long standing hypertension and hyperlipidemia. Her physical examination, electrocardiogram and resting echocardiogram were unremarkable.
-Relevant test results prior to catheterization:
- Relevant catheterization findings:
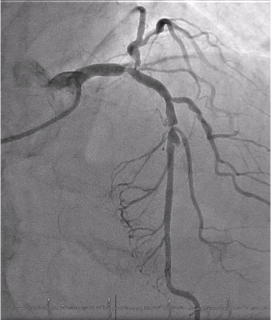
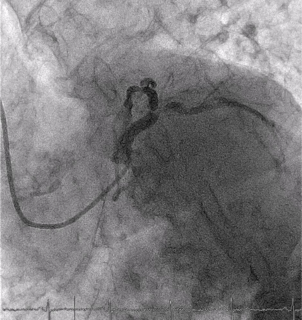
Baseline coronary angiogram1. Left coronary angiogram showed severe distal LM bifurcation followed by severe focal calcified stenosis of mid LAD2. Right coronary angiogram revealed small and non-dominant vessel
   |
|
|
[Interventional Management]
- Procedural step:
A Sheathless 7.5 F JL3.5 was engaged LM via radial approach.The 0.014-inch 180cm Runthrough wire was passed to distal LAD followed by sweeping balloon technique using Mozec SC 3.0 x 15mm from ostial LAD to distal LM for plaque modification. Fielder FC wire was successfully inserted to LCX via Sasuke microcatheter followed by pre-dilation to ostial LCx by 2.5 x 15mm Ryujin balloon. Mid LAD lesion was pre-dilated by 2.0 x 15 mm Ryujin balloon followed by stented with 2.5 x 34mm Resolute Onyx. Distal LM was pre dilated with 3.0 x 34 mm Mozec balloon, then, 3.0 x 14 mm Mozec balloon was anchored at mid LAD. Resolute onyx 3.5 x 18 mm stent was successfully delivery and deployed at LM-ostial LCx. Following angiogram revealed distal stent edge dissection, therefore, LCx was additionally stented with Onyx 2.5 x 15mm. LM to LAD was stented with 4.5 x 22 mm Onyx. Kissing balloon was performed via 3.5 x15mm NC TREK Balloon to LCx and 4.0 x 15mm NC TREK Balloon to LAD. Final angiogram and intravascular ultrasound revealed optimal result.
- Case Summary:
In this case, due to severe angulation of LM to LCx, wiring and stent delivery to LCx were extremely difficult. Balloon sweeping technique and microcatheter were applied for wiring to LCx and balloon anchoring technique was performed for stent delivery.
|
|