Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191108_002
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Mini Crush in Left Main in Patient with Existing Provisional T-Stenting in Left Main and LAD | |
| Raghav Sharma1, Arvind Yuvaraj Narasimhan2, Prathap Kumar Pillai3 | |
| RKM Hospital, India1, Sri Narayani Hospital and Research Center, India2, Meditrina Hospital, India3, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mrs D
-Relevant clinical history and physical exam:
56/F Diabetic & hypertensive underwent PCI with stenting to LAD in 2018 for USAP.5 days post procedure she presented with acute AWMI. Stent thrombosis in LAD. POBA to LAD done. LMCA dissected during procedure (balloon induced) following which patient had a cardiac arrest and then revived. PCI with stenting of left main to LCx done. August 2019, she presented with effort angina. Vitals & basic general physical exam non contributory.
  -Relevant test results prior to catheterization:
All baseline blood investigations were within normal limits. ECG showed Old AWMI with no new/acute changes. Echo - No RWMA. Normal LV function. Exercise stress test (TMT) was positive for inducible ischemia.
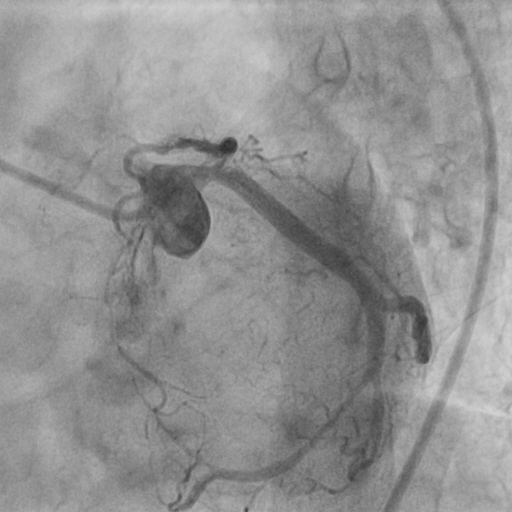
- Relevant catheterization findings:
CAG revealed 80% ISR in LM to LCx stent & LAD ostial 90% stenosis followed by distal stent having another 80-90% stenosis. Distal LAD very small caliber (unsuitable for grafting). However, Patient was advised CTVS opinion for CABG which they refused.
|
|
|
[Interventional Management]
- Procedural step:
7F XB guide catheter engaged to LMCA. LM to LAD crossed with fielder FC PTCA GW.LAD (SB) strut dilated with 1.5mm & 2.5mm NC balloons first. LAD ostium pre-dilated with 3.5mm NC balloon. 2.75*40 DES deployed at 12atm with 2 struts into the LMCA. Another fielder FC PTCA GW was parked distally in the LCx. Over the wire, a 4*16mm DES was taken directly & deployed at 14atm. (Wire from the LAD was removed before stenting to avoid breaking of the wire due to jailing. LAD wire re-crossed and parked distally in LAD. Struts dilated with 1.5mm & 2.5mm NC balloons. Entire LAD stent till the ostium was post dilated. Finally, a kissing balloon dilatation done with a 4*12mm NC balloon in LMCA to LCx stent & 2.75*12m NC balloon in LAD. IVUS was done which showed good opposition of stents & good visualization of the neo carina.
- Case Summary:
Mini crush technique Is ideal in a scenario like this because of presence of double stent strut load. Also, with this technique there is less chance of missing the side branch ostium. Less difficulty in crossing the stent struts compared to conventional bifurcation stenting technique. The main branch stent should be dilated & side branch stent struts should be properly crushed so that the wire can be smoothly crossed through the crushed struts. IVUS guided procedure plays a vital role in this type of case by not only aiding in the visualization of the neo carina but also helps confirming struts are apposed well.
|
|