Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191106_002
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
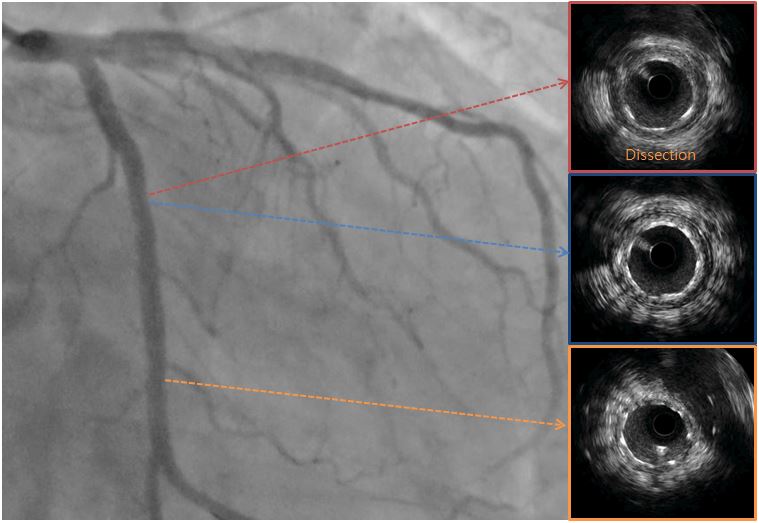
| Spontaneous Coronary Artery Dissection and Scrub Typhus | |
| Kyu Tae Park | |
| , | |
|
[Clinical Information]
- Patient initials or identifier number:
11020117
-Relevant clinical history and physical exam:
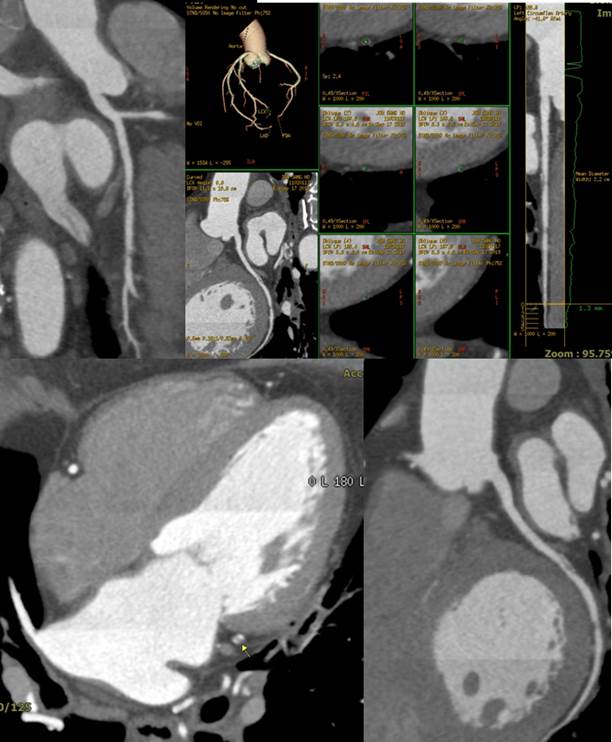
We describe a 58-year-old man with spontaneous coronary artery dissection presenting with chest pain. The patient visited emergency room due to chest pain with fever. Simple chest X-ray, ECG and cardiac marker were normal, so he was discharged with medication. After 2 days later he visited to cardiology with chest pain with chill. Eschar was observed at right chest wall atypically. And coronary CT angiography was performed due to the persistence of the chest pain after initial management, and a spontaneous dissection of the left circumflex artery was observed.
  -Relevant test results prior to catheterization:
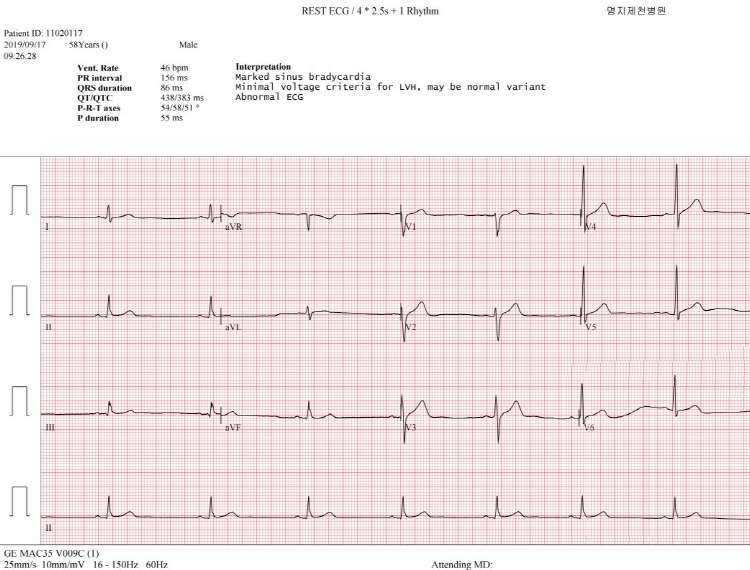
ECG was marked sinus bradycardia(46bpm) and normal cardiac marker.
  - Relevant catheterization findings:
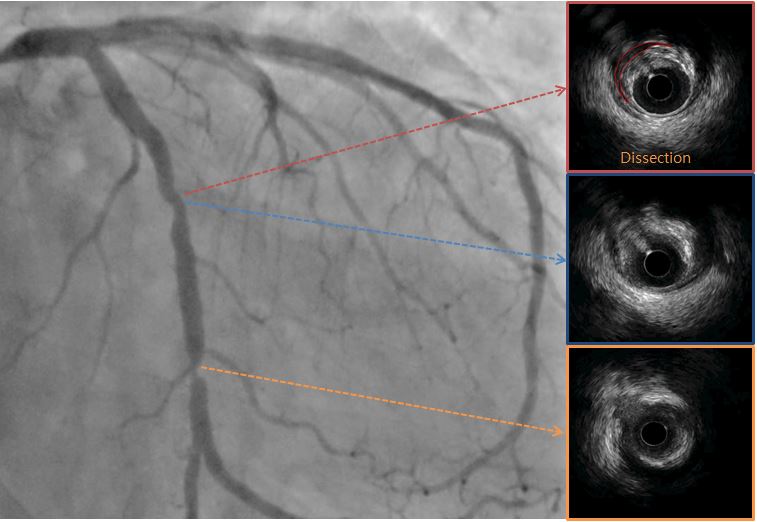
He underwent coronary artery angiography and we performed IVUS and distal severe stenosis lesion with fibrotic plaque and dissection flap were seen. Percutaneous coronary artery intervention (PCI) was done at distal severe stenosis lesion and then dissection lesion with drug eluting stents sequentially. Successful PCI was done and ECG was recovered to normal sinus rhythm. And he was discharged in good condition with medical treatment at the scrub typhus.
|
|
|
[Interventional Management]
- Procedural step:
Coronary angiography (CAG) revealed critical stenosis in distal left circumflex coronary artery (LCx) and mild eccentric stenosis in proximal LCx. We examined intravascular ultrasound (IVUS) for LCX because previous cardiac CT has shown that the dissection flap was in proximal LCx. It revealed large amount of plaque burden in distal critical stenotic lesion and moderate stenosis with fibrotic plaque in dissection lesion. Minimal lumen area (MLA) was about 2.53 mm2 and plaque burden was 74% at distal LCX and MLA was about 3.16 mm2 and plaque burden was 71% at proximal LCx with dissection flap. Firstly, balloon angioplasty was done for proximal to distal LCx using 2.5 x 15 mm balloon catheter, then we implanted 3.0 x 18 mm Xience Sierra for distal LCx and 3.0 x 28 mm Xience Sierra for proximal LCx. We also performed additional balloon angioplasty using 3.0 x 15 mm non-compliant balloon for stent under-expansion. Follow-up IVUS showed good stent apposition and expansion. Final CAG showed good distal flow without residual stenosis.
  - Case Summary:
We described a rare case report with spontaneous coronary artery dissection in man who complained chest pain with infection sign after typhus fever. We successfully identified and treated with coronary artery stenting after cardiac CT and IVUS imaging.
|
|