Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191104_005
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| A Treacherous Bifurcation with a Tight Angulated Side Branch | |
| Tze Ming Chan1, Asri Ranga2, Abdul Raqib Abd Ghani3 | |
| Columbja Asia petaling Jaya, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, Hospital Serdang, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
CKF
-Relevant clinical history and physical exam:
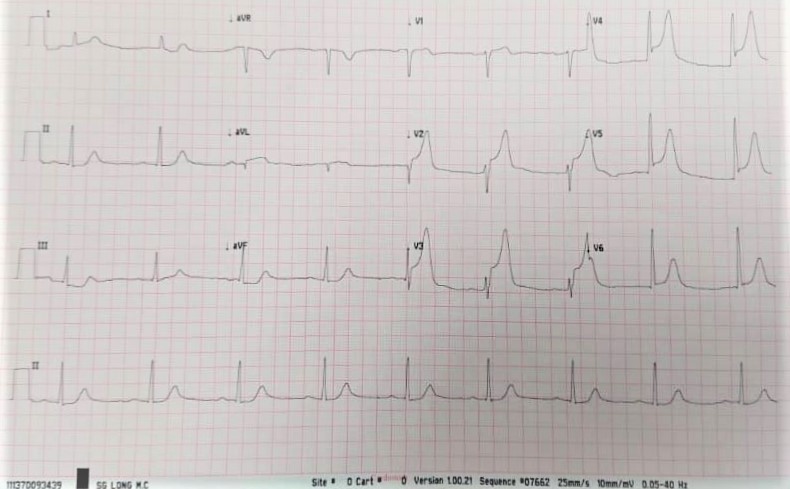
CKF is a 73-year-old male smoker with no previous medical illnesses. Complained of angina at 9 am but worsened at 5 pm. Arrived at the primary centre and performed an ECG which demonstrated ST elevation in V2-V6. IV Metalyse initiated. Post 1 hour, angina persisted with persistent ST elevation. He was then referred to our centre for rescue angioplasty.
 -Relevant test results prior to catheterization:
- Relevant catheterization findings:
LMS: smooth
|
|
|
[Interventional Management]
- Procedural step:
As the Diagonal 1 is a big and important vessel, we decided on a 2 stents strategy using a culotte method. A 6F EBU 3.5 was engaged into the left main with good support. Sion blue wired into LAD with not much difficulties. BMW wire used to wire into Diagonal (Dg) 1, but failed. Changed to a Fielder XTR wire but unsuccessful. After much attempt, we decided to POBA the tight lesion at the bifurcation with a 2.5mm x 15mm balloon to alter the plaque in a hope that it would ease the entry of the wire into DG1. Fortunately, this worked and Fielder XTR was successfully wired into DG1. POBA DG1 with the same 2.5mm X 15mm balloon. Balloon expanded well but had an angle to it. A Promus Premier 3.5mm x 20mm stent was then advanced into the DG1 but was unable to pass through into the DG1. An NC balloon 3.5mm x 15mm was able to pass through and expanded well in the DG junction. However, the stent was still unable to cross through. An anchor balloon technique was deployed using the 3.5mm x 15mm balloon which was anchored in the LAD just distal to the bifurcation but it still failed to deliver the stent through. A Guidezilla was our next strategy. This mother-and-child catheter was advanced all the way into the DG with some effort. Finally the stent was successfully delivered and deployed. POTS done, and LAD wire was removed and rewired back in. Stented LAD with a Promus Premier 4.0mm x 28mm. Rewired into Dg and Kissing balloon inflation was done. Completed with POTS. Good end results.
- Case Summary:
Bifurcations intervention is a complicated enough procedure especially when things do not turn out the way it should. This is a good case demonstrating the difficulty in wiring the angulated stenotic diagonal vessel. Firstly, by predilating the tight LAD, it assists the wire going into the diagonal. Secondly, post predilatation of the diagonal, the stent was unable to passthrough, even after changing wires and using anchor balloon technique. Finally only with a Guidezilla that is deep seated all the way into the diagonal can the stent be delivered. Culotte method was chosen because of the angle and the size of the side branch. An eventful culotte method entails.
|
|