Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191104_002
| STRUCTURAL HEART DISEASE - Others (STRUCTURAL HEART DISEASE) | |
| All Challenges Accepted: Incomplete Balloon Deflation, Stent Migration During (Bail-Out) Subclavian Artery Stenting in a Sick Child with Iatrogenic Subclavian Artery Perforation | |
| Krishna Prasad Nevali1, Krishnasantosh Vemuri2, Bhupendra Kumar Sihag3, Naganur Sanjeev3 | |
| NRI Academy of Sciences, India1, FORTIS HOSPITAL MOHALI, India2, Post Graduate Institute of Medical Education & Research, India3, | |
|
[Clinical Information]
- Patient initials or identifier number:
DK
-Relevant clinical history and physical exam:
6 years old child weighing 15 kg with a diagnosis of hemolytic uremic syndrome and was in need of dialysis.IJV catheterization was attempted without back bleed.CT showed catheter tip not in the lumen, and it was removed leading to massive hemothorax and hemodynamic compromise.Resuscitation done with ICD, multiple blood transfusions, fluids and inotropes.Cardiac services were called upon and percutaneous endovascualr intervention was planned upon as the child was unfit for surgery.
-Relevant test results prior to catheterization:
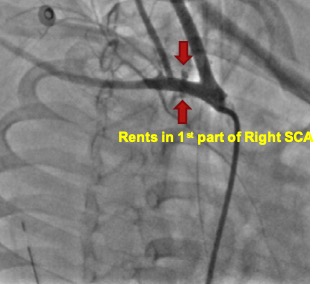
CT angiography showed multiple rents in 1st part of right subclavian artery between common carotid artery and vertebral artery.Distance between right CCA and vertebral artery: 14 mmProximal right subclavian artery 4.8 mm, distally 4.2 mmVertebral system was left predominant
Platelet count was 20 x 109/l 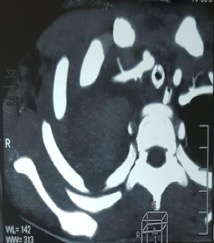   - Relevant catheterization findings:
1. Mediastinal shift to the left due to massive hemothorax.2.Injection into the right subclavian showed dye leak from the junction of right common carotid (CCA) and vertebral artery. Not significant.3. Tamponade effect of hemothorax was thought and ICTD revisioned with higher bore drain.4. Repeat angiography showed increased dye leak from the same point confirming the leak significance.5. Distance between CCA and vertebral artery : 14 mm6. Plan at this point balloon inflation +/- covered stent
 |
|
|
[Interventional Management]
- Procedural step:
1. JR guide, BMW wire parked in distal subclavian2. Prolonged inflation of semi compliant balloons to occlude perforation (to avoid stenting)3. Persistent dye leak depsite inflated balloon. So, planned for stent implantation.4. Incomplete balloon deflation, leading to difficulty in balloon removal. Whole assembly has to be withdrawn and rewired5. Subclavian artery rewired and injection showed persistent dye leak. Hemodynamic parametres were borderline at this point6. So a GRAFTMASTER 4 x 16 mm covered stent was placed across the rent. Persistent dye leak, although less.7. One more hurdle encountered, stent has migrated proximally and placed across the ostium of common carotid artery.8. Guide catheter was slowly pushed to ensure the stent is moved beyond the common carotid and a partially inflated balloon was used to position the stent at the desired position.9. High pressure larger sized balloon inflation was done with 5 x 12 mm @ 20 atm, resulting in good apposition and stable position.10. Repeat angiography showed no dye leak with well expanded stent.11. Post procedural neurological examination was normal.
- Case Summary:
1. USG guidance should be a norm rather than choice for central line catheterization.2. We can tackle perforations with percutaneous approach even in sick children.3. Preintervention CT is always informative in complex vascular intervention.4. Catheterization lab should be well equipped with covered/ peripheral stents and other apparatus.5. Partially inflated balloon helps in repositioning the migrated stent.
|
|