Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_047
| ENDOVASCULAR - Complications | |
| Percutaneous Removal of Dislodged Central Venous Port Catheter: Rendezvous Wire Retrieval Technique | |
| Dharmaraj Karthikesan1, Wirash Kehasukcharoen2, Chee Tat Liew3, Chea Chin Yung1, Lee Kuo Ting4, Sathvinder Singh5, Mohd Ridzuan Bin Mohd Said6, Khor Leet Ming7, Saravanan Krishinan8 | |
| Hospital Sultanah Bahiyah, Malaysia1, Central Chest Institute of Thailand, Thailand2, Pantai Penang Hospital, Malaysia3, Sultanah Bahiyah Hospital, Malaysia4, Hospital Serdang, Malaysia5, Sultan Ahmad Shah Medical Centre, Malaysia6, Hospital Pulau Pinang, Malaysia7, Ministry of Health Malaysia, Malaysia8, | |
|
[Clinical Information]
- Patient initials or identifier number:
RMJ
-Relevant clinical history and physical exam:
A 62-year-old woman with history of rectosigmoid carcinoma (Dukes C) was referred by the surgical team for a dislodged central venous port catheter. She had completed chemotherapy and exploratory laparotomy with Hartmann's procedure. The chemo port was inserted two years prior and during removal it was noted that the port catheter had dislodged.
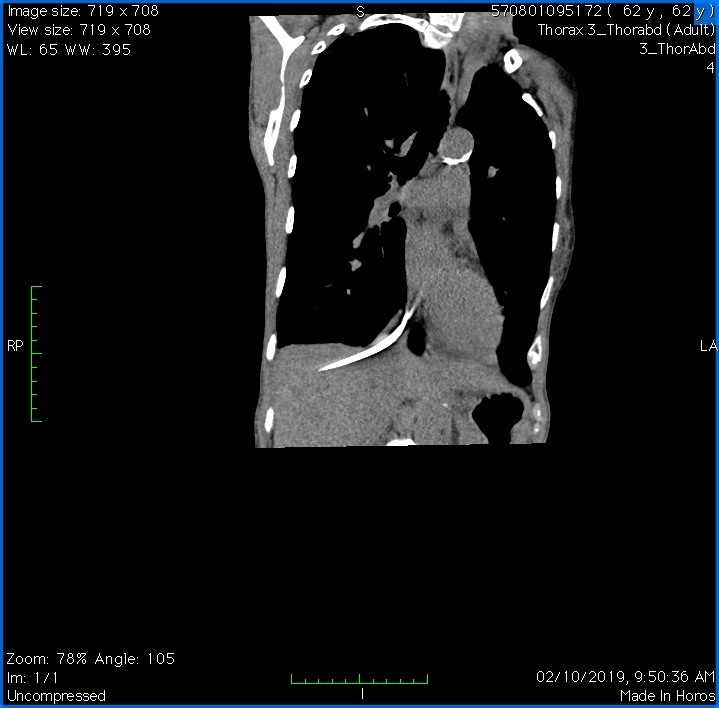
-Relevant test results prior to catheterization:
Chest radiograph confirmed the presence of the dislodged port catheter. Computed tomography (CT) scan showed the catheter lodged in the right atrium extending into the inferior vena cava and right hepatic vein.
   - Relevant catheterization findings:
Using a 10 French right femoral vein approach we first confirmed the presence of the catheter using fluoroscopy. Selective contrast injection showed both ends of the catheter lodged deeply within the hepatic vein and right atrial appendage. It was clear at this point that snaring and retrieval will only be possible if either ends of the catheter was first released and freed up.
|
|
|
[Interventional Management]
- Procedural step:
Attempted first to release the tip lodged in the hepatic vein using a pigtail catheter but failed as the port catheter was lodged in too deeply. We also tried using both homemade snare and the EN Snare system to capture the tip in the right atrial appendage but we were unsuccessful. Even attempting to move the tip with a pigtail catheter while snaring failed. We changed strategy and used a stiffer ablation catheter with a bidirectional tip to catch and release both ends of the port catheter into the inferior vena cava. Using EN Snare via left femoral approach we were able to successfully snare the tip of the port catheter and pull it downwards. With the homemade snare, we caught the other end and pulled it towards the right femoral sheath but during manipulation the sheath was dislodged. We exchanged the left femoral to a new 10 French sheath and used the EN Snare for retrieval. Once again, the sheath was dislodged while pulling the port catheter out. We then railroad a new 10French sheath across the EN Snare which was still gripping the port catheter.Despite multiple attempts using both the homemade snare and EN Snare via both femoral approaches we remained unsuccessful. At this point, we innovated with a rendezvous wiring technique using a Sion Blue wire into the port catheter via JR 3.5. A non-compliant balloon was then inflated which trapped and fixed the port catheter. This technique aligned the port catheter with the femoral sheath allowing it to be retrieved safely.
- Case Summary:
Final angiography results of the iliac and femoral veins showed no perforation or dissection. This case has several learning points. Firstly, it elucidates the usage of the ablation catheters to assist in the retrieval of dislodged central venous port catheters. Secondly, operators should be well versed in the usage of both conventional and homemade snares. Finally, the rendezvous wire and balloon trapping enable safe and easy removal of the port catheters as it becomes aligned to the femoral sheath. To the best of our knowledge, this is the first time this technique has been described and successfully attempted in the retrieval of a dislodged central venous port catheter.
|
|