Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_034
| ENDOVASCULAR - Complications | |
| Bail-Out of Unsuccessful Subclavian Artery Stent Deployment | |
| Ching Way Chen1 | |
| Ntuh Yunlin Branch, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Lin
-Relevant clinical history and physical exam:
This 60-year-old man has underline disease of diabetes mellitus and hypertension under regular medical control. He had intermittent chest pain with left shoulder pain for 10 months. No cold sweating or dyspnea on exertion was noted. Physical examination showed blood pressure difference between upper limbs (left brachial blood pressure 102/79 mmHg; right brachial blood pressure 132/84 mmHg).
 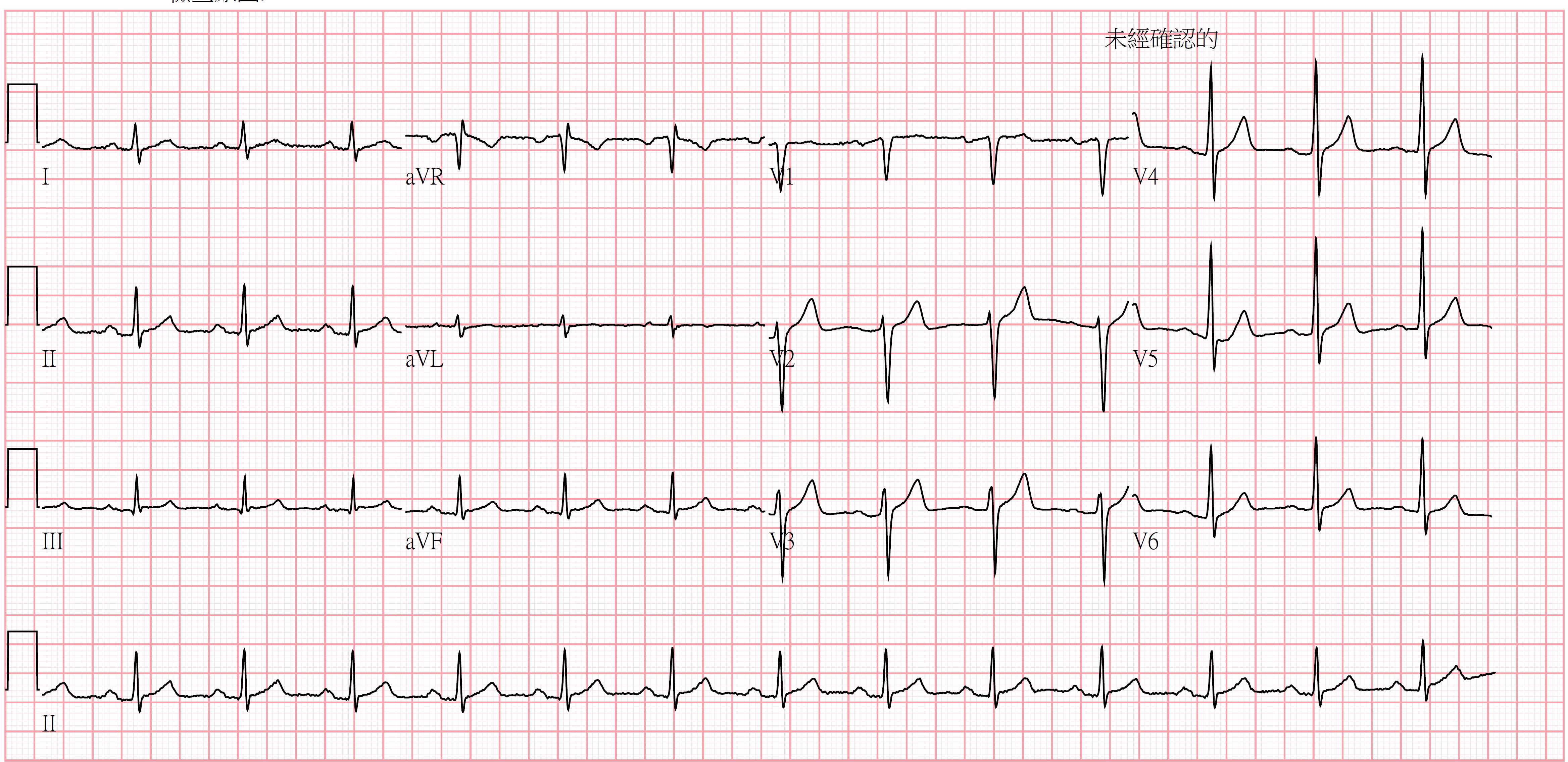 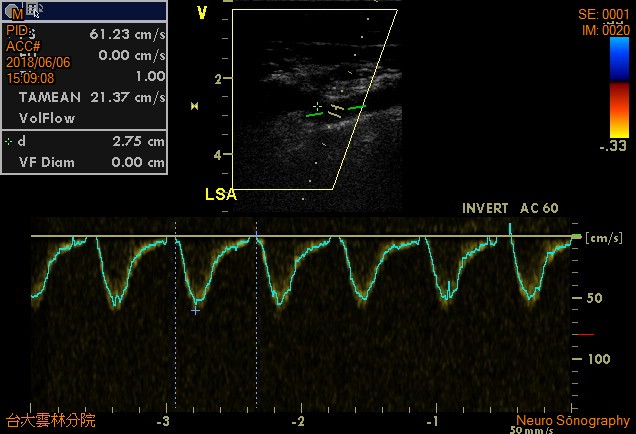 -Relevant test results prior to catheterization:
Chest X ray showed no cardiomegaly. Electrocardiogram showed normal sinus rhythm. Echocardiography revealed good left ventricular contractility without regional wall motion abnormality or valvular heart disease. Vascular duplex revealed monophasic waveform over left subclavian artery with left subclavian stealing phenomenon.
- Relevant catheterization findings:
Coronary angiography via right femoral artery showed patent coronary arteries. Left subclavian artery angiography revealed proximal 80% stenosis with pressure gradient over 40 mmHg between aorta and distal left subclavian artery.
|
|
|
[Interventional Management]
- Procedural step:
We engaged left subclavian artery with JR4 8Fr. guiding catheter and then passed Terumo 0.18 wire to distal left subclavian artery. Percutaneous transluminal angioplasty with peripheral balloon Sterling 6.0*20mm up to 10atm10". We then passed Boston Express iliac stent 7.0*27 mm to left subclavian artery. However, stent balloon ruptured during stent deployment. Only proximal part of the stent was expanded. Distal part of stent could not open. Stent balloon could not advance to distal un-expanded part of the stent. Thus, we decided to pull back the not-fully expanded stent with stent balloon and withdraw the system to right iliac artery. No peripheral balloon could not pass the stent. We used CXI micro-catheter to pass through not-fully expanded stent to switch Terumo 0.18 wire to coronary wire Fielder FC. We expanded the stent with coronary balloon Tazuna 2.0*15 mm. We deploy the stent at right iliac artery with peripheral balloon Mustang 6.0*20mm and 8.0*20 sequentially. Final left subclavian artery showed improved flow without obvious dissection. Pressure gradient decreased less than 10 mmHg after percutaneous transluminal angioplasty above.
- Case Summary:
This case demonstrated how we could deal with unexpanded stent due to balloon rupture during stent deployment. Sequential angioplasty with smaller balloon and even coronary balloon may help to expand the stent. Thus, we avoid surgical removal of the un-expanded stent through cut-down method. We also avoided vascular damage or rupture during advancing the stent balloon or peripheral balloon with larger diameter comparing to sequential expanding with coronary balloon first.
|
|