Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_031
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| Successful EVT with Central Crossing Technique to Common Femoral Artery with Calcified Nodule | |
| Hirokazu Tanaka1, Akinori Sumiyoshi2, Atsunori Okamura3, Mutsumi Iwamoto1, Satoshi Watanabe1, Hiroyuki Nagai4, Masato Ishikawa1, Kota Tanaka1, Satoshi Suzuki1, Kenshi Fujii1 | |
| Sakurabashi Watanabe Hospital, Japan1, Sakurabashi Watanabe Advanced Health care Hospital, Japan2, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan3, Saint Joseph's Translational Research Institute, USA4, | |
|
[Clinical Information]
- Patient initials or identifier number:
T.K
-Relevant clinical history and physical exam:
Previously he was performed PCI to LAD and has a hypertension and DM.70s years old male with an intermitted claudication of his left lower limbs, and a Rutherford classification of gradeI-2 was admitted to our hospital.
-Relevant test results prior to catheterization:
His rest ankle brachial index (ABI) score of his left limb was 0.55. Echography showed the left common femoral artery has a severe stenosis with a severe calcification. Peak systolic velocity (PSV) was 5.02. Peak systolic velocity ratio (PSVR) was 14.5.
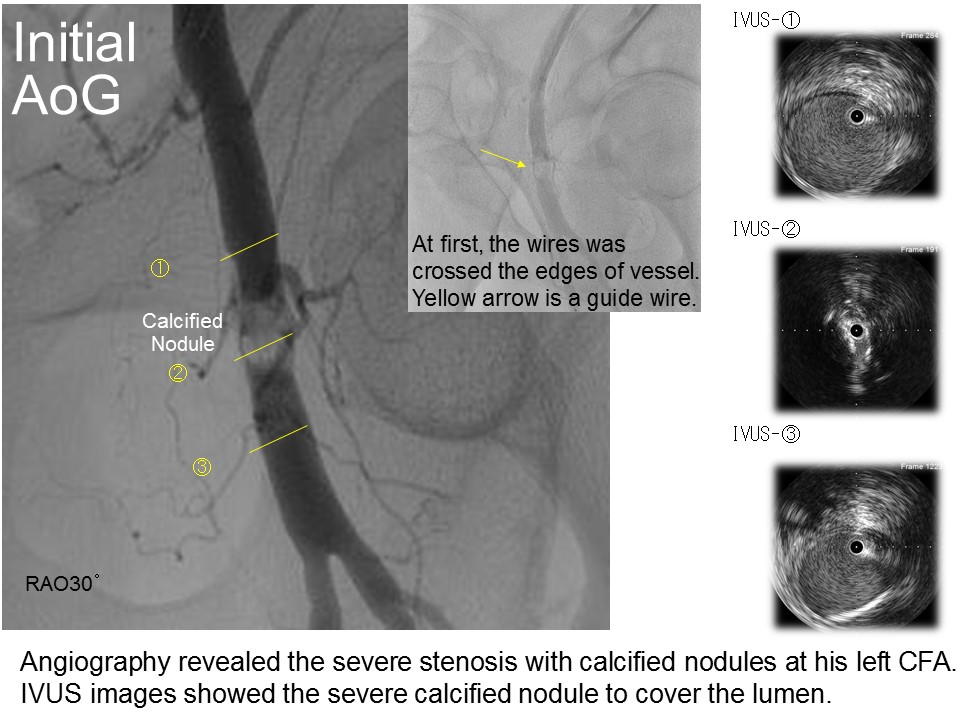 - Relevant catheterization findings:
Angiography revealed the severe stenosis with calcified nodules at his left CFA.
 |
|
|
[Interventional Management]
- Procedural step:
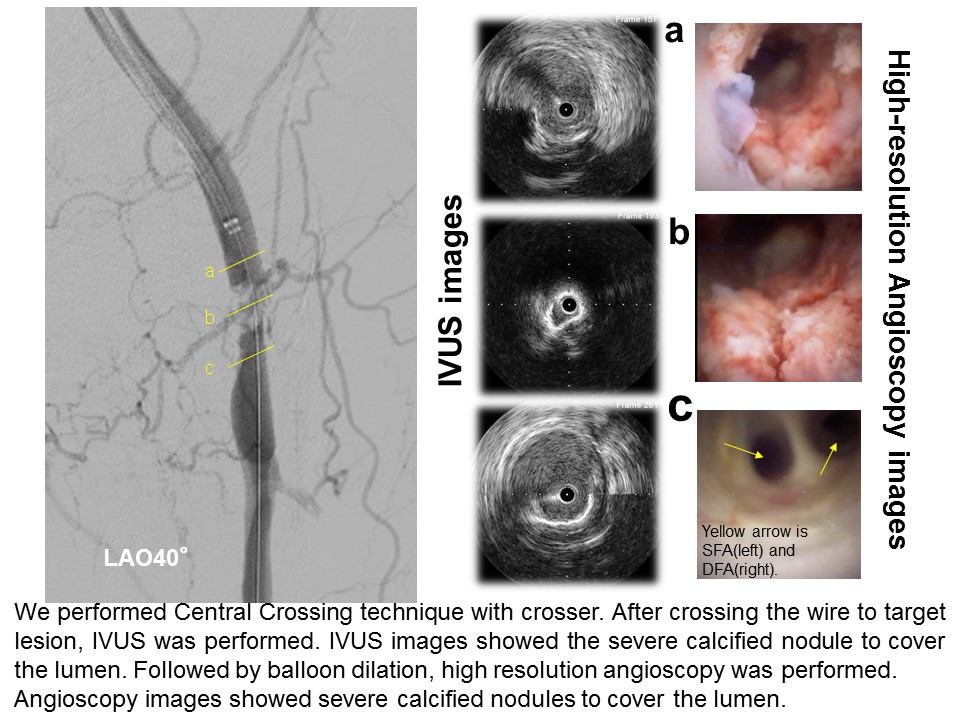
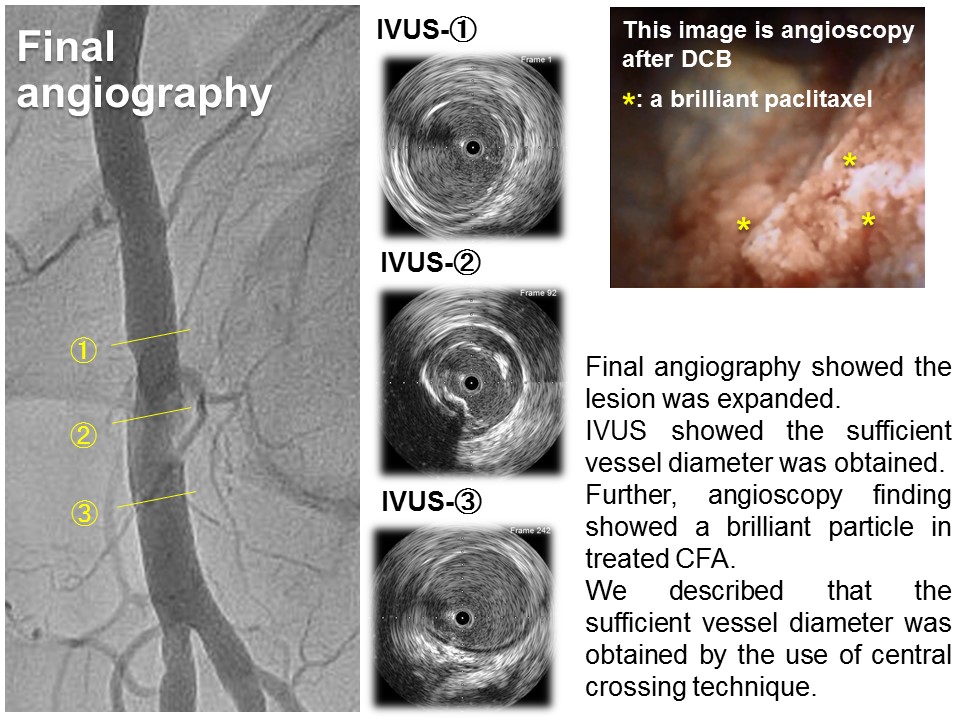
Therefore, we performed EVT with 6Fr JR4.0 guiding catheter into 6Fr parent sheath through his right femoral artery. We tried to cross the target with GladiusMG14 PVESTM (Asahi Intecc). However the wire was not crossed, we changed the wire to a 0.014 inch stiff wire (Astato XS 9-40TM (Asahi Intecc)) and a 0.014 inch super stiff guide wire (Jupitar MAX TM (Boston Scientific)). So, the wires was crossed into the calcified nodule with Central Crossing under CrosserTM (BD Bard). After crossing the lesion, IVUS was performed. Because the lesion has a severe calcs, IVUS did not pass the lesion. Therefore, we performed POBA with 2.0mm high pressure balloon (JADETM (Orbus Neich)), followed by checked the lesion. IVUS images showed the severe calcified nodule to cover the lumen. These IVUS images was not clear to evaluate the lesion characteristic. To assess the lesion characteristic, high-resolution angioscopy was used. Angioscopy images revealed clearly the severe calcified nodule to cover the lumen. We thought that if POBA was performed with normal balloon, the lesion could not be dilated in this situation. Therefore, 4.0mm scoring balloon was used and followed by 6.0mm non-compliant balloon (DORADOTM (BD Bard)). After dilation, we used 6.0mm Drug Coated Balloon (IN.PACT ADMIRALTM(Medtronic)). After DCB, we checked the target vessel with high-resolution angioscopy. Angioscopy finding showed a brilliant particle in treated SFA. Final angiography showed the lesion was expanded.
 - Case Summary:
When EVT was performed at a common femoral artery, the treat of a stent less is necessary. However, wires often cross the edges of vessels, making it difficult to get a sufficient vessel diameter. In this case, we tried to cross into a calcified nodule with Central Crossing Technique by crosser and sufficient vessel diameter was obtained. We describe the use of high-resolution angioscopy and IVUS to evaluate calcified nodule lesions after treatment with central crossing technique.
|
|