Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_014
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Balloon Assisted Reverse Wiring Technique for LMCA Bifurcation PCI | |
| Minh Hung Ngo1 | |
| Choray Hospital, Vietnam1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr D
-Relevant clinical history and physical exam:
The patient has just noticed angina pectoris CCS class 3 for 3 months. He is on optimal medical treatment, however, angina tends to be worse. He was then recommended to undergo functional or imaging test to have some more information for treatment. His medical history is normal and CVRFs are smoking, hypertension and dis-ipidemia. Nothing special is noted on clinical examination.
-Relevant test results prior to catheterization:
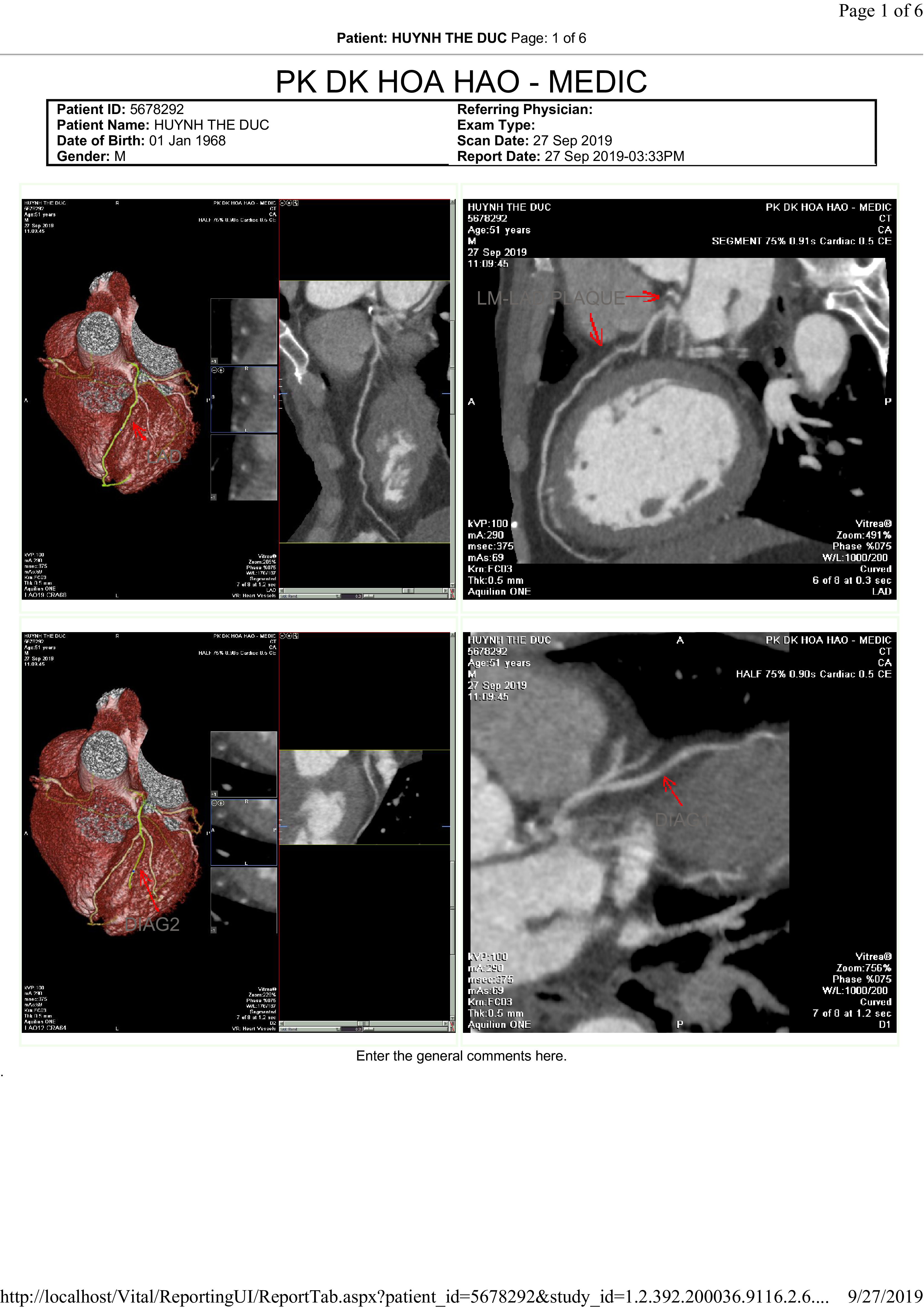
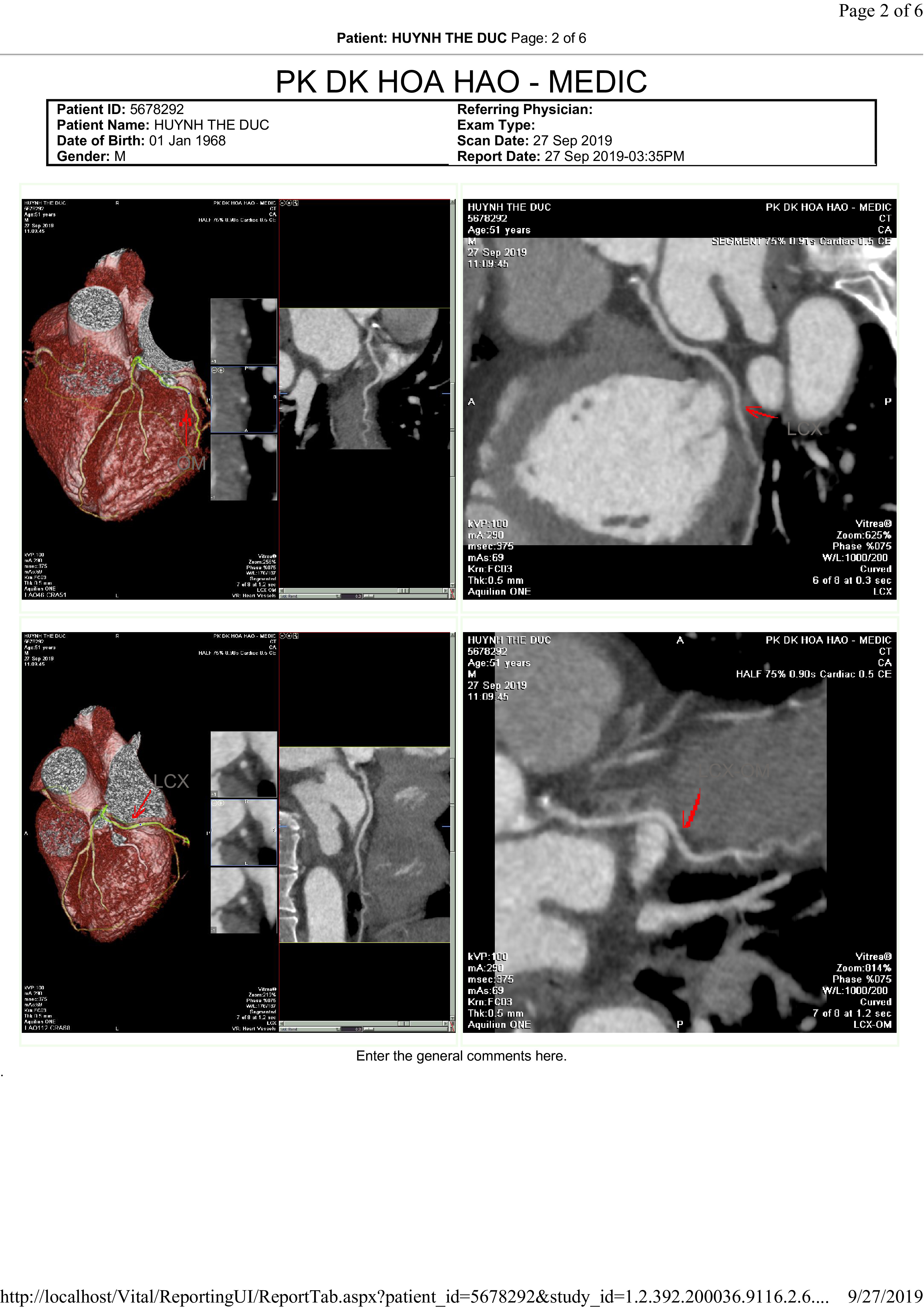
His coronary artery MSCT shows very a tight lesion at distal LMCA and another tight lesion at ostium of proximal LAD.
  - Relevant catheterization findings:
His coronary artery angiography shows very a tight(90%) lesion at distal LMCA and another tight (90%) lesion at ostium of proximalLAD. The angulation between distal LMCA and proximal segment of LAD is about120 degrees. Medina Classification is (1-1-0). There are minor diseaseselsewhere on angiography. Based on MSCT and current angiography, the angulationis unfavorable for conventional percutaneous coronary intervention.
 |
|
|
[Interventional Management]
- Procedural step:
The LMCA and proximal LAD lesions were first tried with a run-through guide wire however, it failed to cross after multiple attempts. The next steps were escalated with Fieder XT, Gaia I loaded inside double lumen catheter (Crusade) using reverse wiring technique which assisted by the double lumen. However, these wires could not cross the proximal LAD lesion because of a big angle between LMCA and LAD (about 120 degrees). Another reason was that the proximal LAD lesion was very tight hence the reverse wire could not easily passthrough as the technique's theory and they were kept prolapsing into ramus and small side branch. An idea was then develop to stop the prolapsing and luckily succeeded to cross the lesion. The rest of procedure was then performed as normal manner.
 - Case Summary:
Conventional reverse wiring with microcatheter (single or double lumen) is still standard technique for wiring obtuse angulation at bifurcation.Balloon assisted reverse wiring technique is a new approach for very tight lesion at exit of bifurcation and when conventional one does not work.
|
|