Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191031_007
| ENDOVASCULAR - Aorta Disease and Intervention | |
| Rare Case of Secondary Hypertension: MID-Aortic Syndrome | |
| Sumanta Shekhar Padhi1 | |
| Raipur-MMI Narayana Superspeciality Hospital, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
MRS SS
-Relevant clinical history and physical exam:
37 YR LADY WAS FOUND TO HAVE VERY HIGH B.P. during evaluation of constant head ache. Clinical examination showed Radio-Femoral delay, no Radio-Radial delay. BP difference of 70 mmHg between upper and lower limb.CBC and RFT were normal. DOppler showed significant folw reduction and near laminal flow in Abdomenal Ao and Renal A. Fundus was Normal.Infalamtory markers were normal.
   -Relevant test results prior to catheterization:
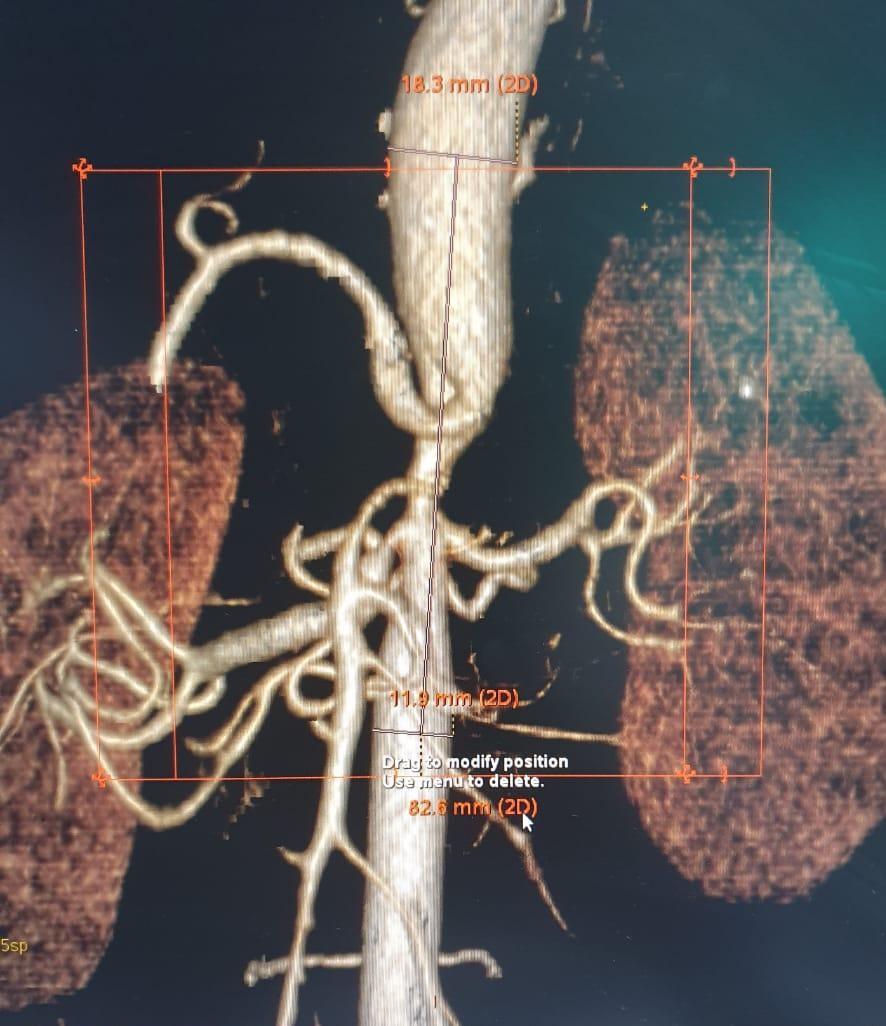
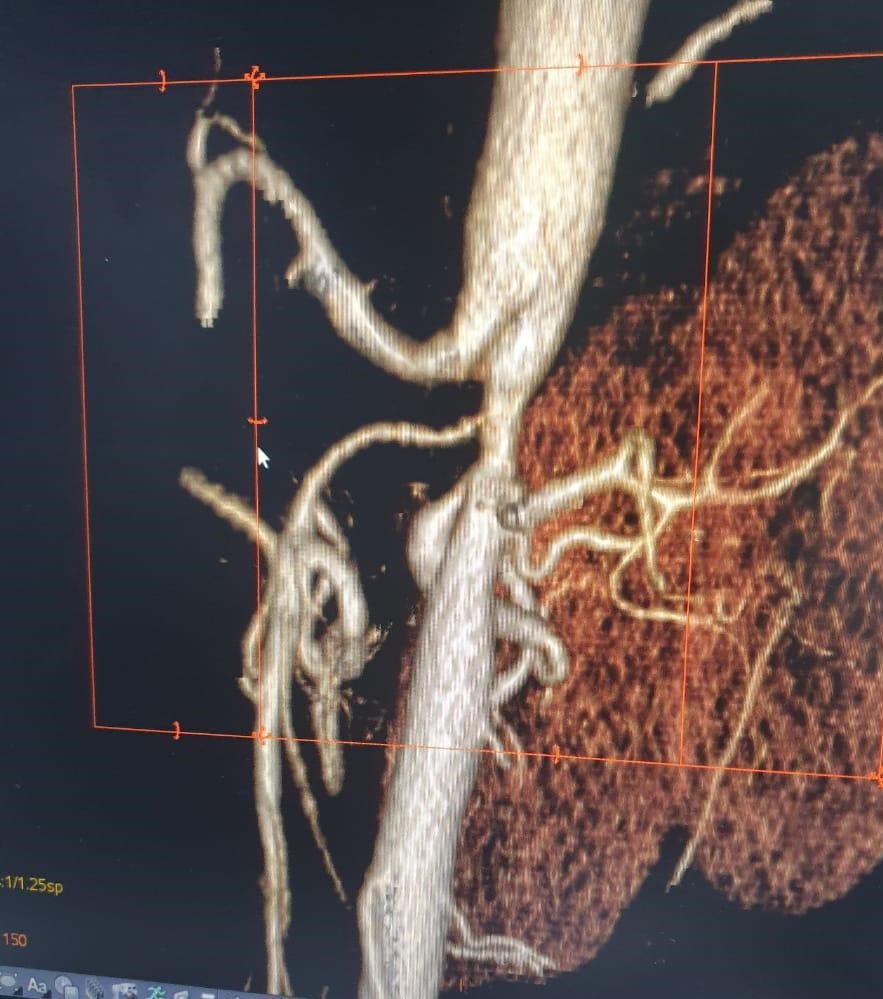
CT angio showed, the abdominal aorta across the origin of both renal A was significantly narrow. The total leght of the narrowing was ~ 82mm,The diamater of normal segment at the upper segment was 14mm and in lower end was 11mm. The nawwoest part was 4mm in diameter. The origin of the Rt renal A and superior mesentric A were significantly stenosed. The Left renal A was normal.
- Relevant catheterization findings:
The pullback gradient across the stenosis was 60mmHg. There was significant Dampening of pressure with 6F cathter in the Rt renal A.
|
|
|
[Interventional Management]
- Procedural step:
The renal A was dilated with 5 x 15mm Balloon. Since there was no significant residual stenosis or dissection it was not stented.Since there was no h/o abdominal angina- nothing was done for the Celiac a stenosis. The abodominal Ao was stented with 14 x 100 mm self expanding stent.Immediate Post stent the gradient was about 40 mm Hg.The residual stenosis at the mid segment was post dilated with a 10 mm balloon twice.There was residual gradient of 16mmHg. Even though there was anatomic residual stenosis there was near complete hemodynamic correction.
- Case Summary:
careful physical examination can give clue for cause of secondary hypertension. Even though abodominal Ao CoA is a rare cause of secondary hypertension appropriate and adequate treatment can gratifying result in managing cases like this.
|
|