Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_028
| CORONARY - Complications | |
| Small Test & Oops! | |
| Kien Chien Lim1 | |
| National Heart Institute, Malaysia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
WLT
-Relevant clinical history and physical exam:
Mr WLT, a 54 years old gentleman with previous history of angioplasty to left anterior descending artery (LAD) and right coronary artery (RCA) presented with stable angina.Systemic examinations were unremarkable. Vital signs stable.
-Relevant test results prior to catheterization:
ECG showed sinus rhythm.2D ECHO demonstrated satisfactory ejection fraction of 50%. Stress myocardial perfusion revealed ischemia at the right coronary (RCA) and left circumflex artery (LCx) territories.
- Relevant catheterization findings:
Left main artery: NormalLeft anterior descending artery (LAD): Severe in stent restenosis mid LAD stentLeft circumflex artery (LCx): Severe stenosis proximal LCxRight coronary artery (RCA): Severe stenosis at proximal RCA
   |
|
|
[Interventional Management]
- Procedural step:
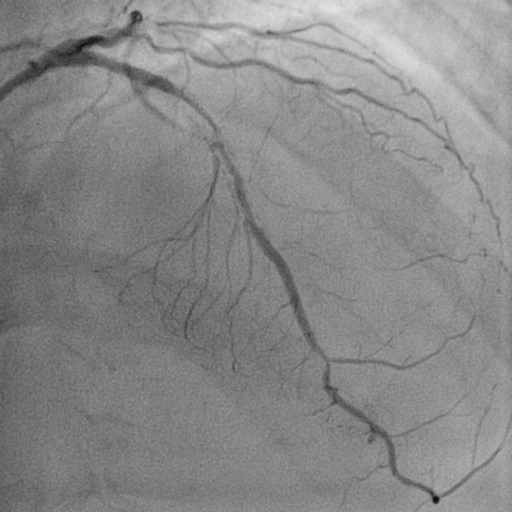
Calculated SYNTAX score of 11. The Option of bypass surgery was offered but was declined by patient. We proceeded with multivessels PCI. RCA then LAD & LCx. We had difficulty to engage the ostial RCA with JR 3.5 6Fr guide catheter. SAL 0.75 6Fr guide catheter provided good guide support and Run through Floppy wire was advanced across the lesion. The proximal lesion was prepared with semi-compliant balloon 2.0 x 15mm and 3.0 x 15mm. There was non- flow limiting dissection at the proximal RCA and thus we decided to stent up to the ostium. A few shots were taken to ensure adequate ostium coverage!While deploying the stent, the stent slipped and a huge dissecting pouch appeared during the small test shot! Oops!
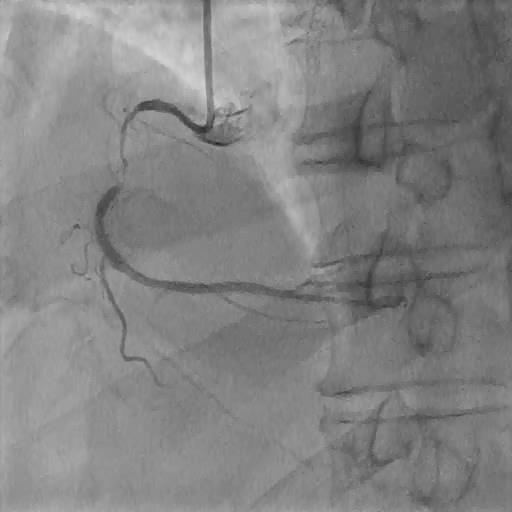
To make the situation worse, we loss our guide and wire! Then reengaged with JR 3.5 5 Fr and rewired after several attempts. Finally, we stented the proximal segment ostium with overlapping stent. The final results was good, TIMI III flow.   - Case Summary:
Our Patient developed peri-procedural myocardial infarction with transient ST elevation at the inferior leads.CT Aortogram performed on the second day showed short segment dissection (1cm) at proximal ascending aorta anteriorly.
A straight forward PCI to RCA which turned out to be a complicated proximal RCA, right coronary cusp (RCC) dissections. The proximal RCA dissection was induced by catheter, while the ostium and RCC dissections was caused by the confirmatory contrast puff during the stent deployment. The learning point are 1)The appropriate guide catheter selection and 2) Very careful ‘small test’ while deploying a stent at the ostium. Preferably being puffed by the main operator. |
|