Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_008
| CORONARY - Chronic Total Occlusion | |
| Today's Complexities Demand Greater Simplicity - Right Coronary Artery Ostial Chronic Total Occlusion (CTO) by Retrograde Technique Using a Handmade Snare by Bilateral Snuffbox Approach | |
| Swapnil Dhondibhau Mate, Chiung-Jen Wu4 | |
| , Kaohsiung Chang Gung Memorial Hospital, Taiwan4, | |
|
[Clinical Information]
- Patient initials or identifier number:
5232203
-Relevant clinical history and physical exam:
A 79 years old gentleman with hypertension, prior history of CVA and Coronary artery disease. Patient had history of percutaneous coronary intervention with Drug eluting stents(DES) to ostium of Right coronary artery(Nobori 3.5 x 14 mm) and PLB (Nobori 3 x 24 mm) 3 years back and another DES (Ultimaster 3.5 x 17 mm) to ostial RCA instent restenosis 2 years back. Now patient presented with chronic stable angina since 6 months
-Relevant test results prior to catheterization:
Echocardiogram showed normal chamber dimensions, no regional wall motion abnormality with good left ventricular systolic function(67%). treadmill electrocardiogram test was strongly positive with Bruce protocol at 4.5 METS with ST changes in inferolateral leads with delayed receovery of changes.
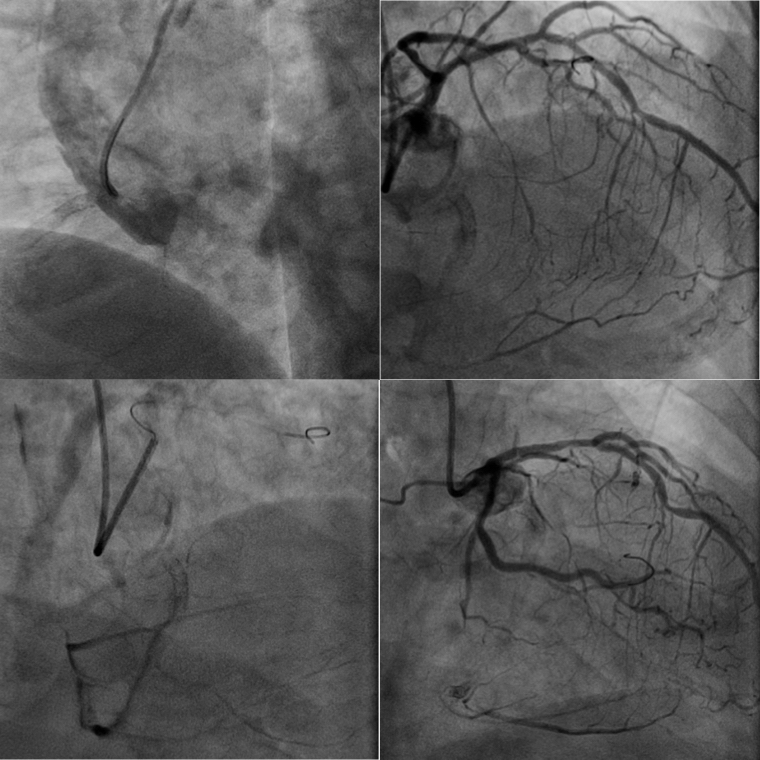
- Relevant catheterization findings:
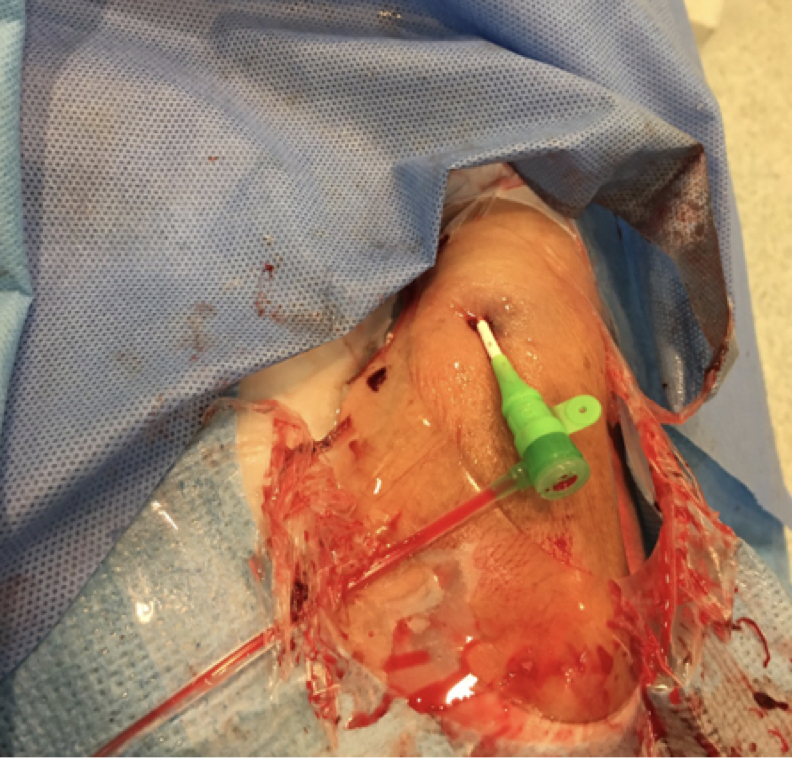
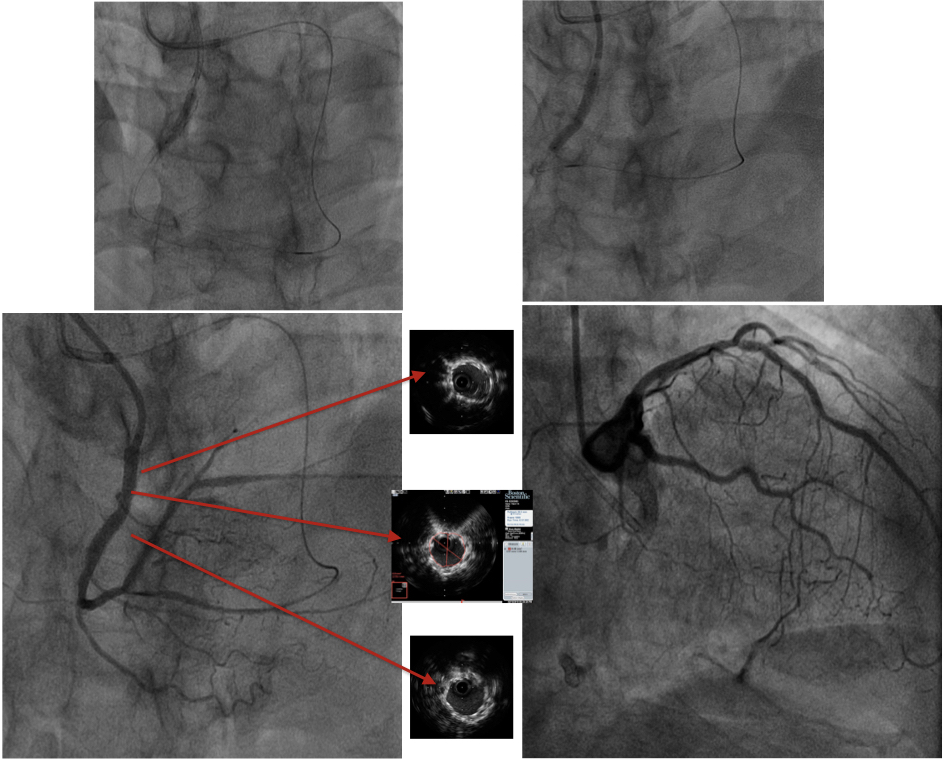
Catheterization was done through left distal radial artery(snuffbox artery) with 6 french Ikari left 4.0 guiding catheter. It showed instent chronic total occlusion at RCA ostium with distal vessel filling via grade III collaterals from left system. J-CTO score was 2. Left system was normal. majority collaterals were septal collaterals from LAD (Three major visible collaterals seen)
  |
|
|
[Interventional Management]
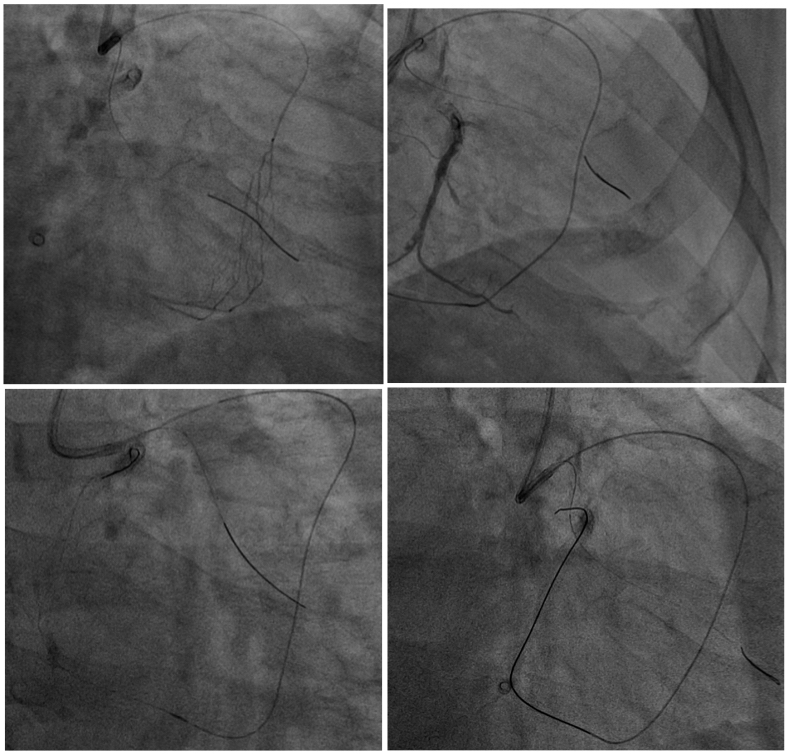
- Procedural step:
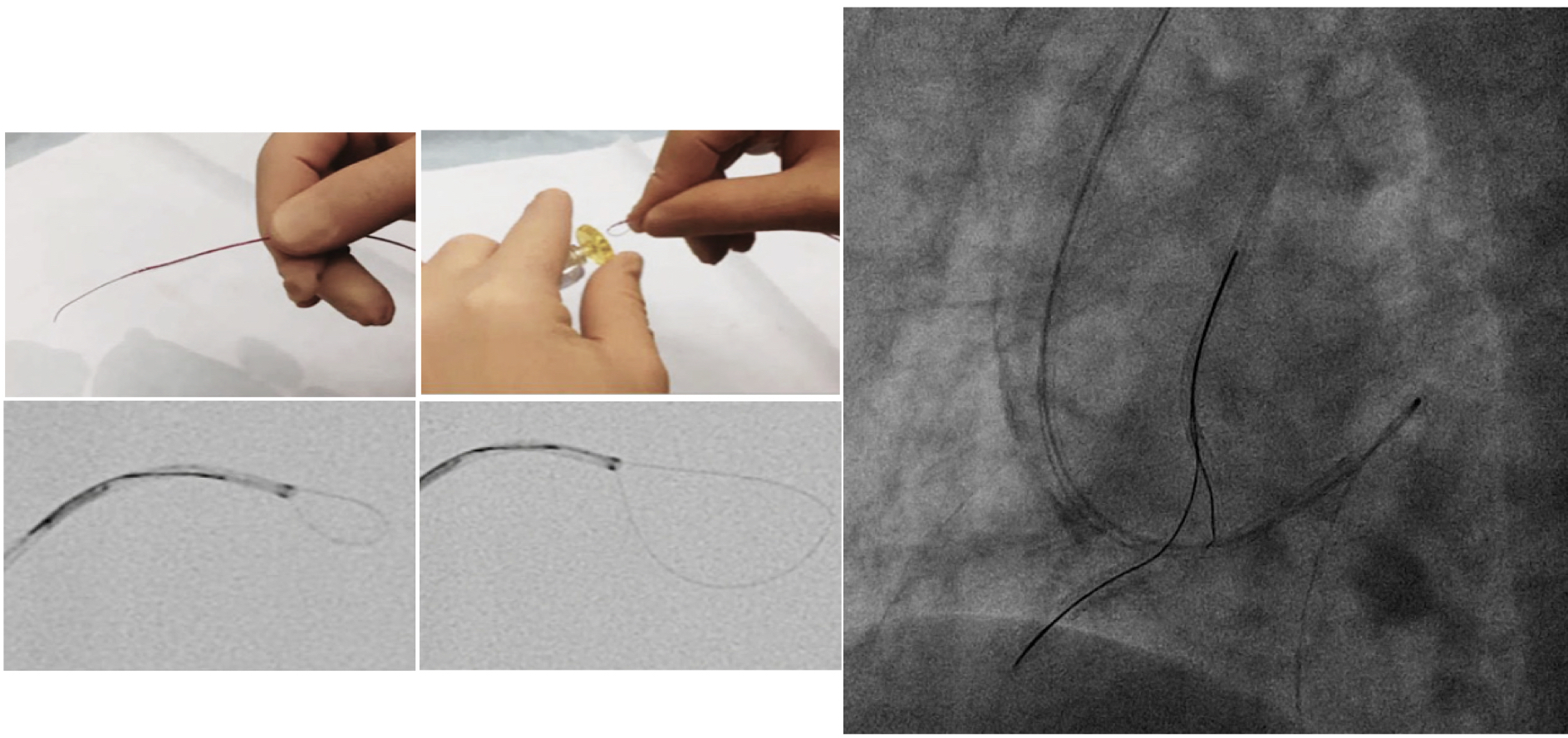
Due to ostial location of chronic total occlusion and absence of stump, retrograde approach was preferred. With a 7 French EBU 4.0, A Sion wire was advanced to PDA in a Finecross microcatheter through one of the septal collateral. Finecross was exchanged for Caravel microcatheter as the former could not cross septal-PDA junction. A Ultimate bros 3 wire could cross the CTO segment to enter in aortic root. through left distal radial artery access a 6 French Judkind right 5.0 catheter was placed in aortic root. A MINITREK 2.5x20 mm ballon was advanced into a 5 in 6 ST01 HEARTRAIL II catheter over Runthrough wire. About 3 cm wire ti was made into a handmade snare by looping and trapping the wire besides the balloon inflated at 12 atm. this assembly was passed to aortic root inside 6 F JR catheter and the UB 3 wire was snared by pulling and catching the wire. The snared wire was stuck inside the snare, which was resolved by pull and push technique after connection a wire extension to the UB 3 wire. Later the Caravel microcatheter was advanced inside the JR catheter and externalisation wasdone using RG3 wire. After predilation with 3.5 mm balloon, a drug eluting stent of size 3.5 x 28 mm was deployed at ostium to proximal right coronary followed by postdilation with 4.0 mm non-compliant balloon at upto 20 atm. Check intravascular ultrasound showed well apposed stent with no stent edge dissection. TIMI 3 flow and 15% residual stenosis was achieved.
   - Case Summary:
|
|