Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191030_004
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| Retrograde Peroneal Artery Puncture for Distal and Superficial Femoral Artery In-Stent Total Occlusion and Rotational Atherectomy in Below-the-Knee Severe Calcified Vessels | |
| Nai-Yu Chi1, Po-Chao Hsu2, Tsung-Hsien Lin2, Ho-Ming Su2, Wen-Chol Voon2 | |
| Kaohsiung Municipal Ta-Tung Hospital, Taiwan1, Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Hou
-Relevant clinical history and physical exam:
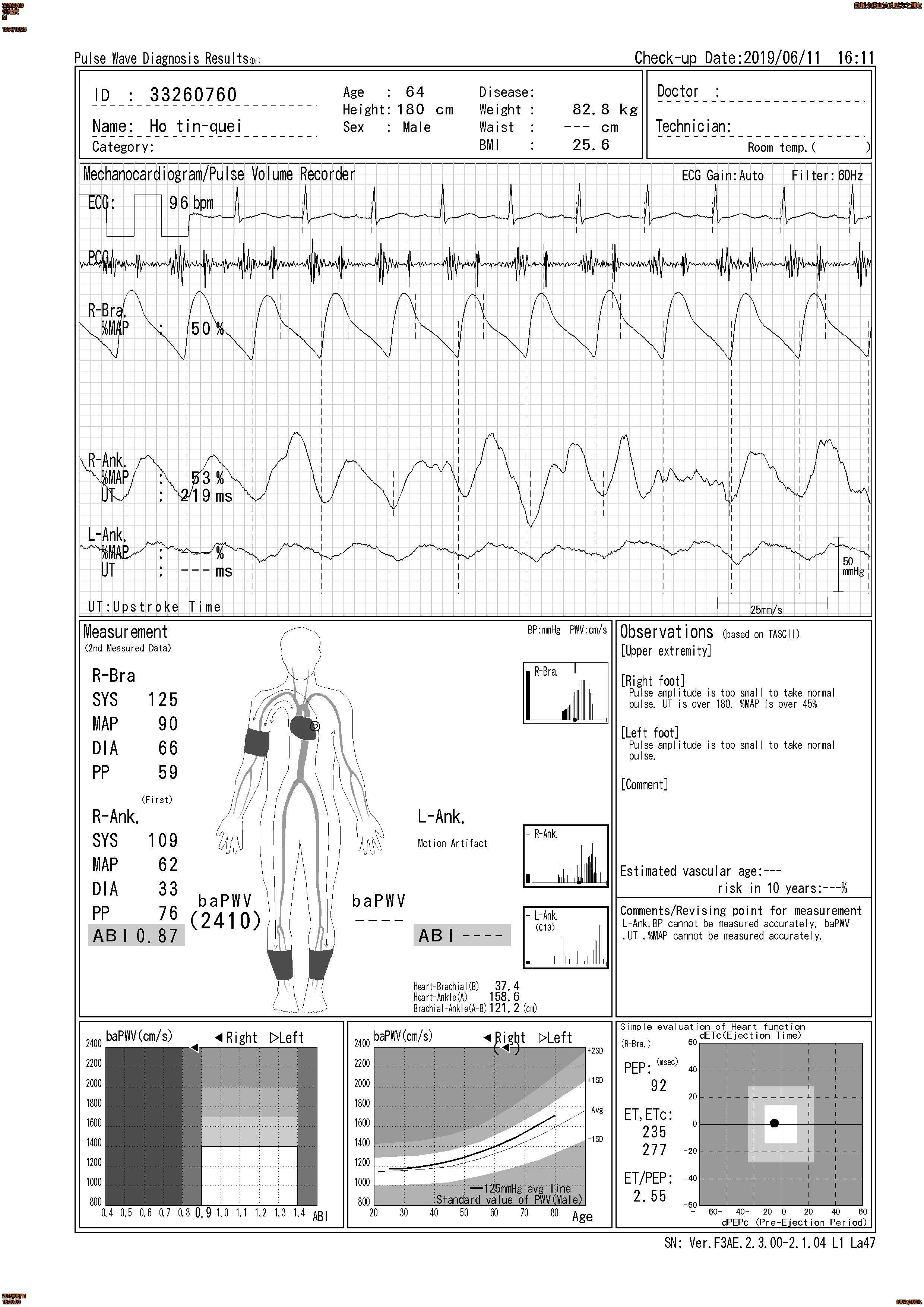
64 year-old man has CAD, (s/p CABG in 2011), ESRD under hemodialysis, T2D, HTN, Hyperlipidemia and Bilateral PAD (s/p stenting in left distal SFA on 2019/1/7 by previous hospital). Due to worsening low limbs painful and cold sensation recently, patient visited our clinic for help on 2019/06/11ABI showed right was 0.87 and left side was not detected. However, left foot has bulla formation on 2019/06/18, patient visited our emergent departmen. We were consulted for intervention.
-Relevant test results prior to catheterization:
ABI showed right was 0.87 and left side was not detected.
 - Relevant catheterization findings:
Angiography before intervention showed Both common iliac a patent, Left external iliac a patentLeft SFA diffuse stenosis and in stent total occlusionLeft Popliteal a (P2/P3) non-significant stenosisLeft ATA 100% occlusion / left PTA 100% occlusionLeft Peroneal artery: non-significant lesion Poor left distal foot run-off
|
|
|
[Interventional Management]
- Procedural step:
In first Session, we used bi-direction approach with cross-over approach with 0.035 wire under CXI support and retrograde approach by puncturing peroneal artery by flow guiding and vessel calcified. We using V18 wire to go into popliteal artery and successfully performed externalization from CXI microcatheter. Peripheral intervention with 5 x 80 mm balloon in SFA and Popliteal artery and then stenting with Supera stent (6 x 120mm) in Middle SFA to popliteal a. Then we managed BTK vessles, we treated ATA first, but our balloon could not pass through ATA middle portion. We then perfromed PTA angioplasty and improving distal foot run-off flow. We stenting Bare metal stent (6 x 80mm) in proximal SFA lesion and closed first session. 2 months, we used Rotational atherectomy (ROTA) for ATA lesion, we finally sent long balloon into ATA distal part and got very good left foot distal run-off.
- Case Summary:
1. For CKD patient, calcified vessels were frequently noted and puncture according to calcification location is a good way to decrease contrast amount also2. Retrograde approach with micropuncture set is frequently needed for tough BTK intervention=> we should be familiar with the retrograde technique
3. For cases with severe calcified BTK vessels, even balloon could not pass through the lesion, Rotational atherectomy (ROTA) is another good choice to recanalize the vessel |
|