Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191029_007
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| Exploration of Image: The Key Role of Optical Coherence Tomography in Identifying an Atypical Unstable Angina Pectoris | |
| Hehe Cui, Hui Chen3 | |
| , Beijing Friendship Hospital, China3, | |
|
[Clinical Information]
- Patient initials or identifier number:
DJR
-Relevant clinical history and physical exam:
A 57-year-old postmenopausal woman was admitted to hospital because of no-cause intermittent chest pain without symptoms of exertional angina for one week. She has a history of mild hypertension and dyslipidemia for 5 years under lifestyle and diet control, and a smoking history (cessation for 10 years). Her younger brother was attacked by acute myocardial infarction in his 50s. Her physical examination was unremarkable.(Bp 138/66 mmHg, heart rate at 53 bpm, no vital positive sign)
-Relevant test results prior to catheterization:
Cardiac troponin T, Cardiac troponin I, N terminal pro B type natriuretic peptide and creatine kinase-MB tests were negative. Echocardiogram showed good ejection fraction (78 %) and no wall motion abnormalities. Her electrocardiogram was normal. A non-invasive coronary computed tomographic angiography (CTA) showed an atherosclerotic plaque with a moderate stenosis in the proximal left descending artery (LAD). No obvious stenosis was found in other coronary arteries.
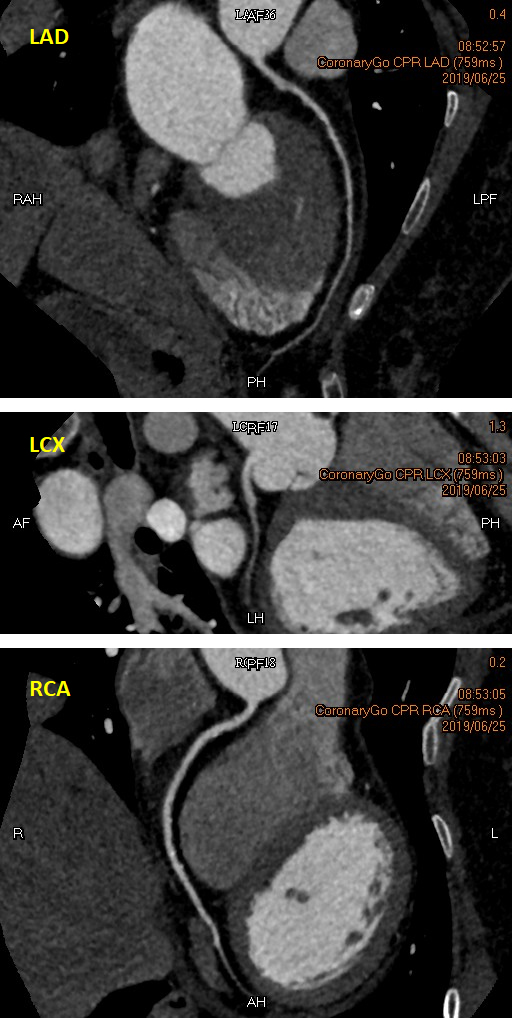 - Relevant catheterization findings:
Although the coronary CTA showed mild lesions, the patient insisted to be examined by a coronary angiogram (CAG) because she was frightened by the heart attack on her brother. The CAG showed a 50 % - 60 % stenosis in the proximal to mid LAD, a normal left circumflex artery, and an atherosclerotic plaque without obvious stenosis in the proximal right coronary artery.
|
|
|
[Interventional Management]
- Procedural step:
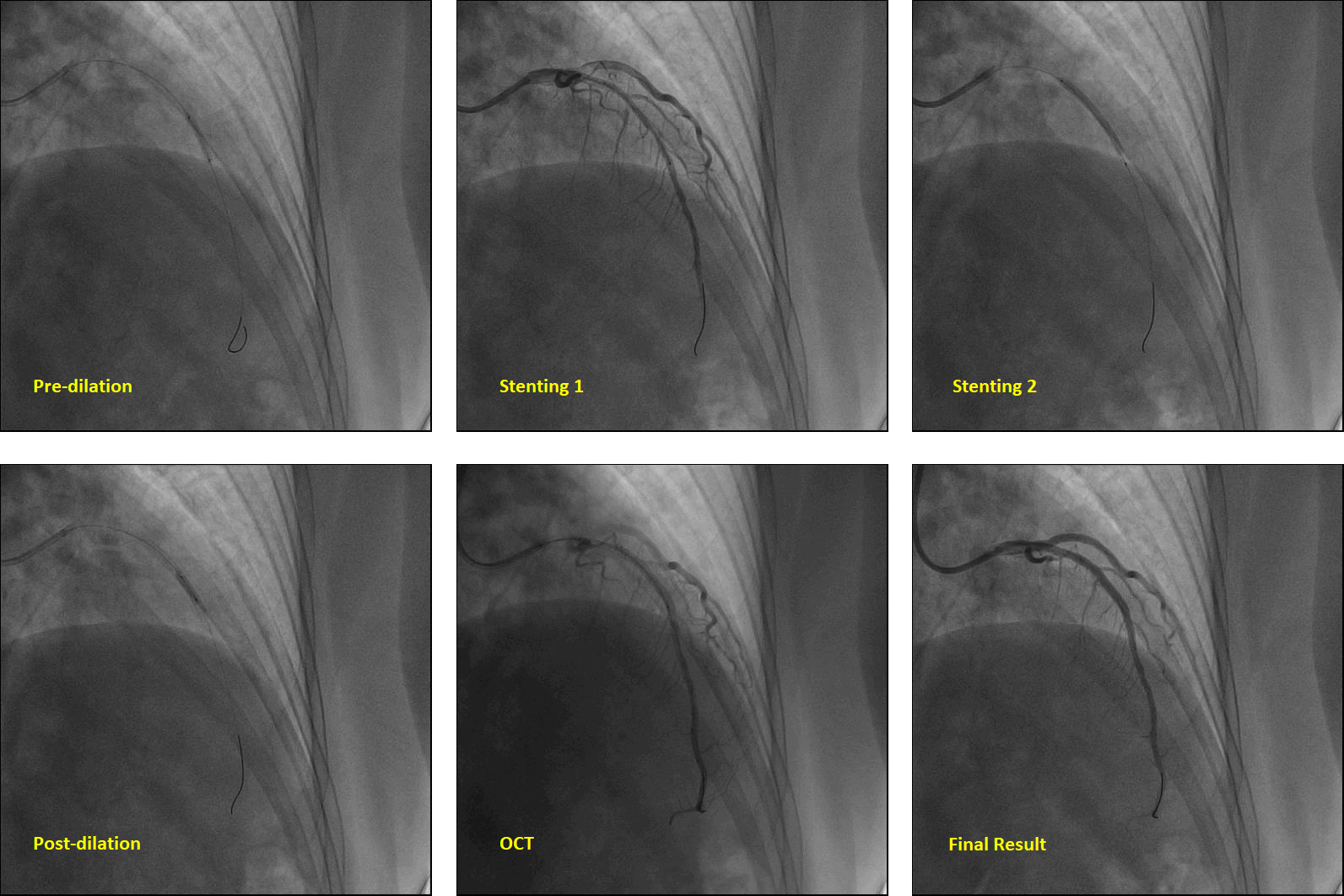
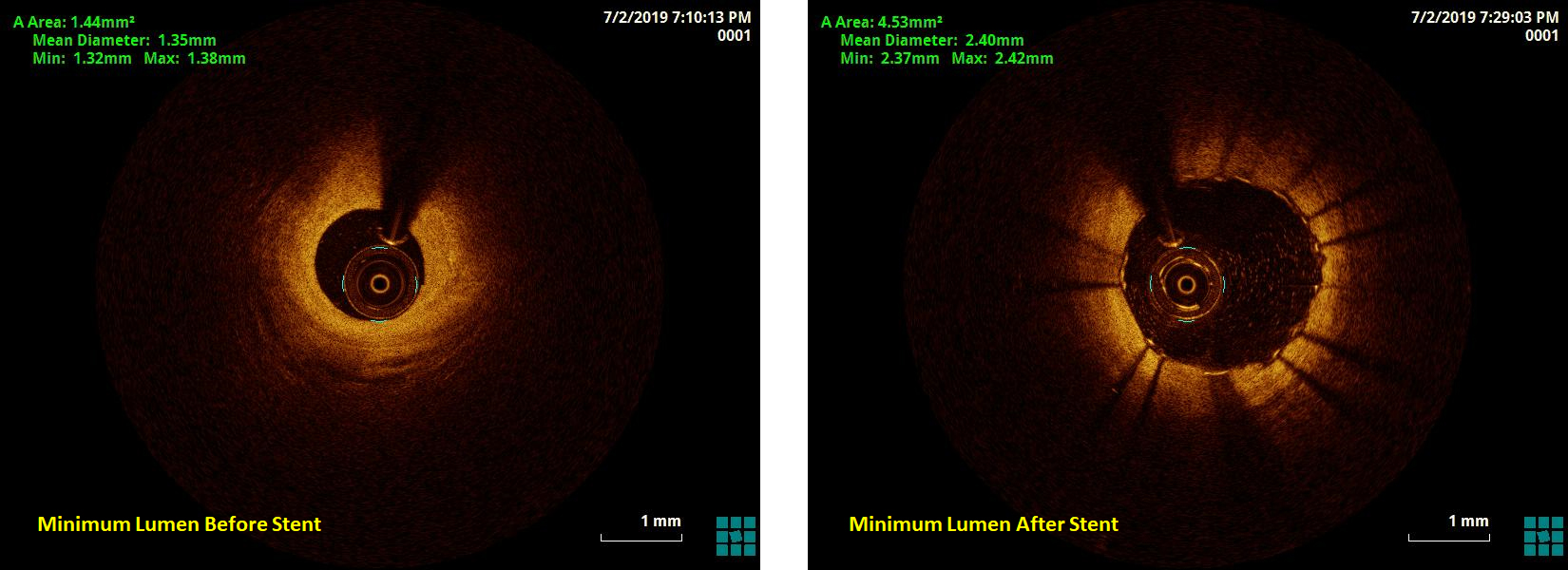
We performed optical coherence tomography (OCT) to clarify the borderline lesions in LAD. The result found a surprisingly severe stenosis in the proximal to mid LAD. The minimum area is only 1.44 mm2 (77% narrowing of proximal reference lumen), the mean diameter is 1.35 mm. The lesion is a mixed plaque with a fibrous cap, some lipid content, a little calcification and intraplaque vasa vasorum as the OCT movie showed. Then revascularization was performed. A pre-dialation balloon (2.5 * 15 mm, Cordis, Hialeah, Florida 33014, United States) was used for predilation at 10 atmospheric pressure (atm). A stent (2.5 * 32 mm, Promus PREMIER, Boston Science, Marlborough, MA 01752) was deployed at 8 atm into the proximal to mid LAD, and a non-compliance balloon (2.75 * 9 mm, NC Sprinter, Metronic, Minneapolis, MN 55432) was used to post-dialate the stent at 16-18 atm. OCT image after stenting showed the minimum intra-stent lumen area was 4.53 mm2, and the stent was well attached.
  - Case Summary:
During follow-up, the patient complained the symptoms were completely relieved. Optical coherence tomography provides a superior resolution (10 μm) of plaque morphology. Compared with CT and angiogram, Additional use of intracoronary imaging techniques facilitates the diagnosis of coronary artery disease and the management of lesions in uncertain cases.
|
|