Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191027_010
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| LCX Ostium - The Achilles Heel of PCI, Will OCT Have an Impact? | |
| Jimmy George P1, Jabir Abdullakutty2, Rony Mathew2 | |
| Lisie Hospital, India1, Lisie Heart Institute, India2, | |
|
[Clinical Information]
- Patient initials or identifier number:
FJI
-Relevant clinical history and physical exam:
A 69 years old gentleman had presented with chronic stable Angina of 1 year that had progressed to Class II in the past I month.He had no risk factors and his ECG was normal, Echocardiography showed no regional wall motion abnormality with fair LV function.A stress testing was done and was positive at 9.6 METS.
-Relevant test results prior to catheterization:
- Relevant catheterization findings:
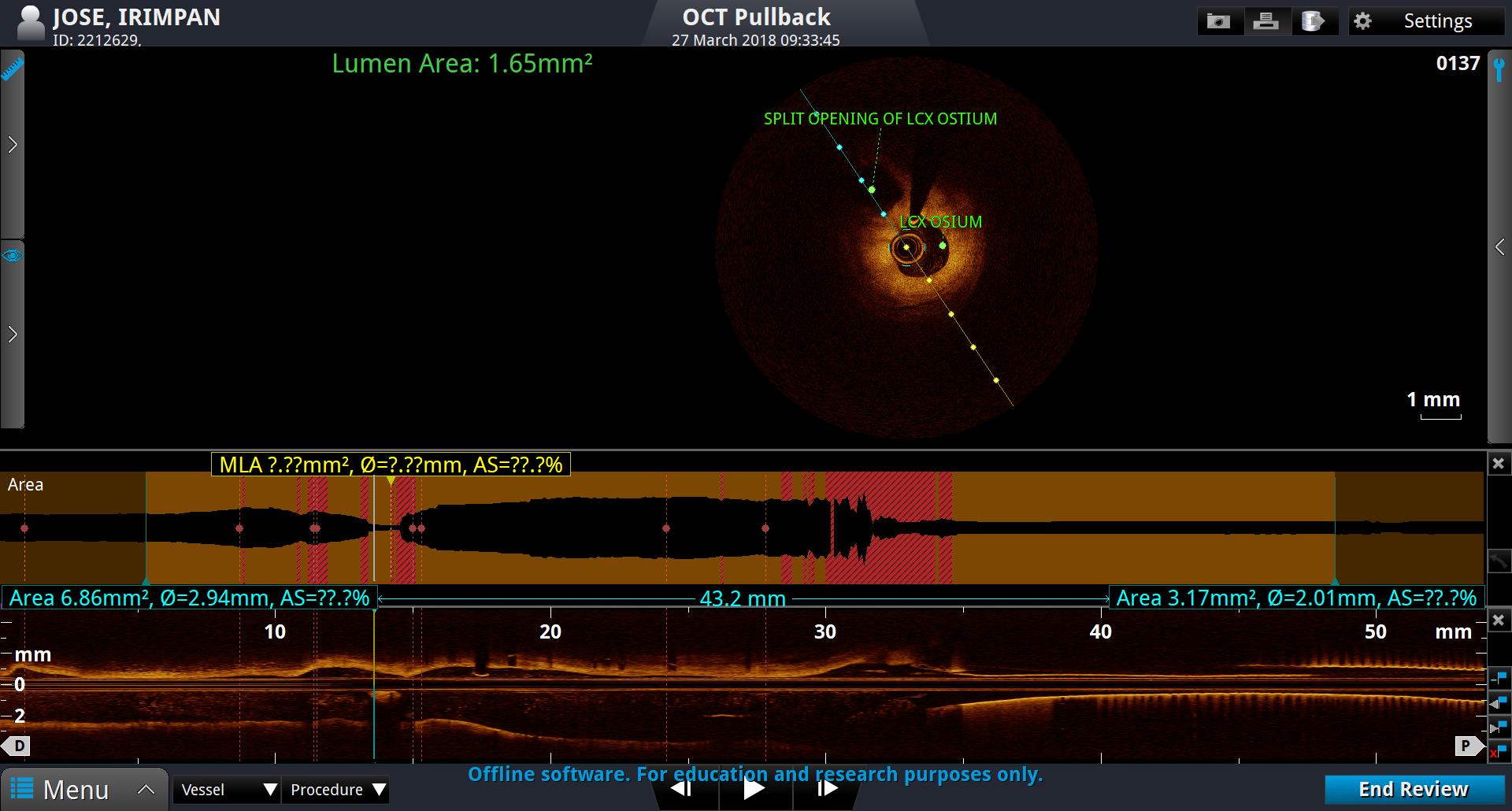
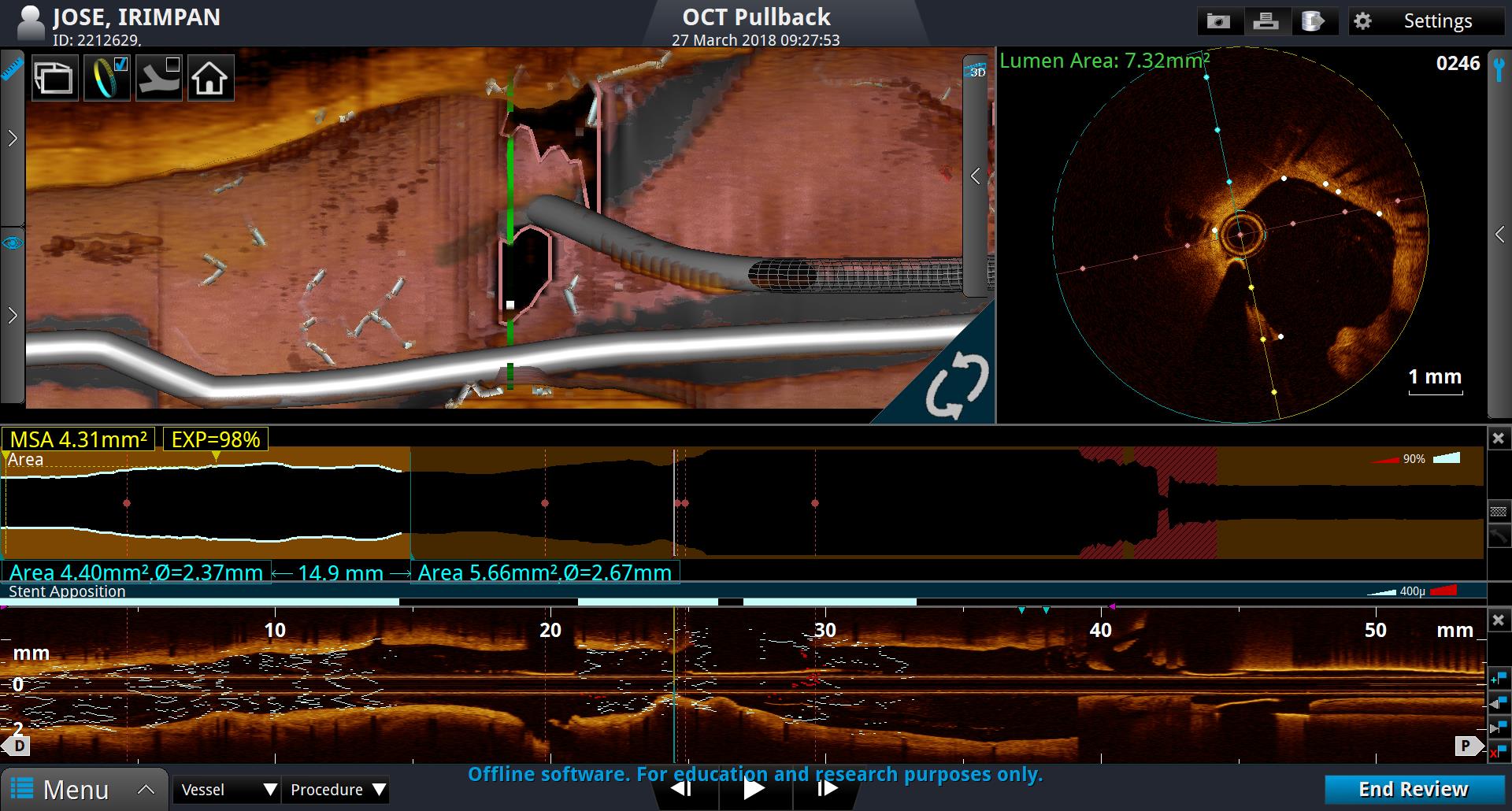
HIs CAG showed distal LM plaquing with proximal LAD 70 % stenosis. He underwent LM-LAD crossover stenting (3.5 X 23 DES) with sparing of LCX ostium under OCT guidance. He was doing well for 2 years later got admitted with rest angina and elevated cardiac markers . His CAG showed patent stent with Ostial LCX ? thrombus, OCT imaging showed red thrombus with ostial LCX significant narrowing. He underwent TAP bifurcation stenting to LCX with a2.75 X 13 DES and SKS balloon dilatation.
 |
|
|
[Interventional Management]
- Procedural step:
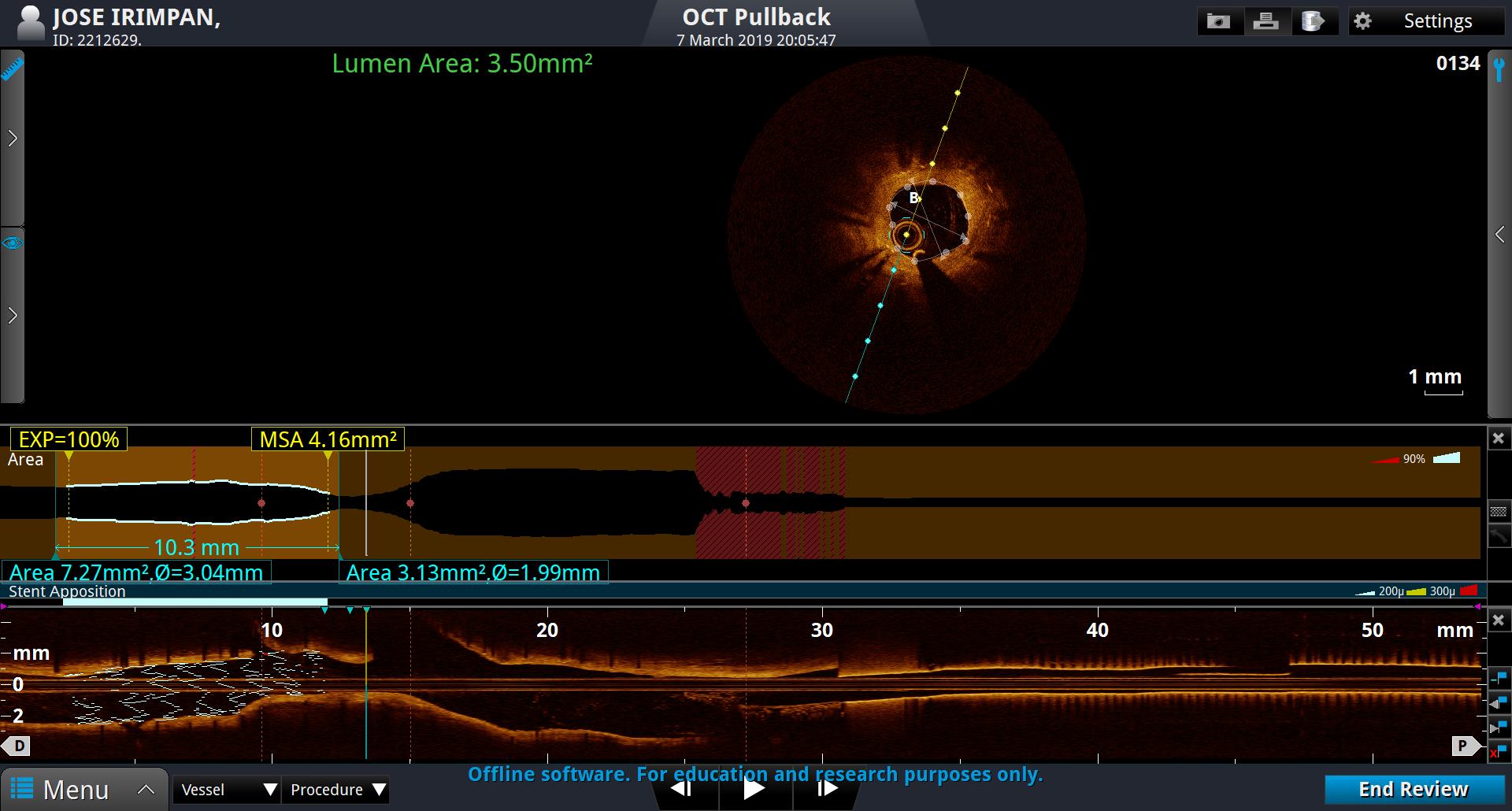
He had now undergone LM crossover stenting in 2016, followed by NSTEMI in 2018 and under OCT guidance had to undergo TAP stenting to LCX with good result. But things did not end there he again presented with postprandial angina and his stress testing was mildly positive at 10.6 METS. Angiogram showed narrowing of ostilal LCX and this time again OCT imaging showed mild neointimal proliferation of LCX ostium with an areaof more than 3.8. An FFR was done to LCX which showed 0.88 and IFR of 0.94, hence he was managed conservatively.
 - Case Summary:
LCX Ostium is always prone to restenosis. In the first LM-LAD crossover stenting LCX carina was well imaged angiographically and intravascular imaging torule out any ostilal and carina issues. But when he presented again OCT showed significant thrombus and restenosis of LCX osmium, hence had to go ahead with bifurcation stenting. The third time in 2019 he had neointimal proliferation but angiographically, Imaging and Physiological (FFR) results were favouring medical management. He was continued on Optimal Medical Therapy.
|
|