Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191023_001
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Direct Coronary Stenting Culminates in Unanticipated Coronary Perforation: Result of Accidental Aggressive Post-Dilatation of Underexpanded Stent with High Pressure NC Balloon | |
| Vipin Thomachan1, Ahmed Siddiqui1, Abdulla Shehab2, Ali Shamsi1, Nawas Mohammed3 | |
| Tawam Hospital, United Arab Emirates1, Burjeel Royal Hospital, United Arab Emirates2, Al Ain Hospital, United Arab Emirates3, | |
|
[Clinical Information]
- Patient initials or identifier number:
SKB
-Relevant clinical history and physical exam:
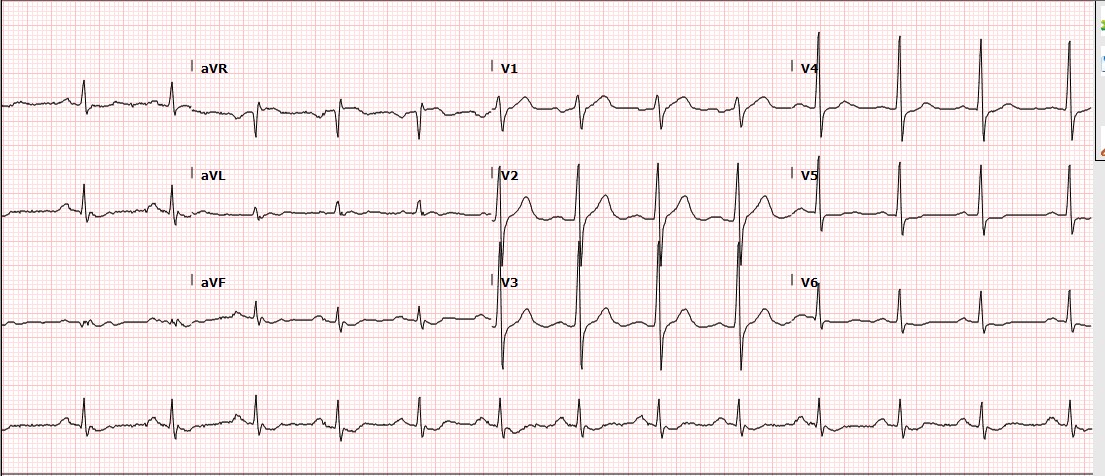
61 year old male patient with history of smoking and dyslipidemia presented with Acute coronary syndrome- Non ST elevation myocardial infarction (ACS-NSTEMI).No similar history in the past or any other associated comorbidities. Clinically patient was stable.
   -Relevant test results prior to catheterization:
Cardiac hs-Troponin T was elevated. Normal Renalfunction. Echocardiography showed LV EF 55% with inferior hypokinesia.
   - Relevant catheterization findings:
CAG showed tota lthrombotic occlusion of proximal RCA and 70% stenosis of mid LAD. RCA lesion was treated with a DES. LAD lesion looked simple and hence stented directly with one DES.
   |
|
|
[Interventional Management]
- Procedural step:
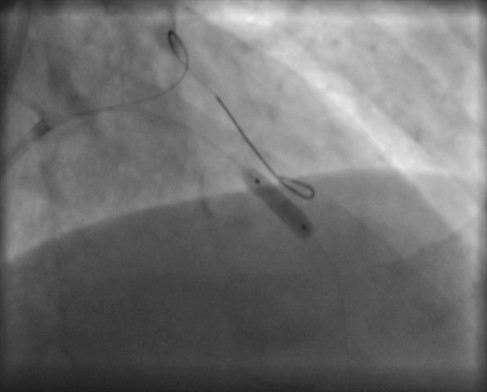
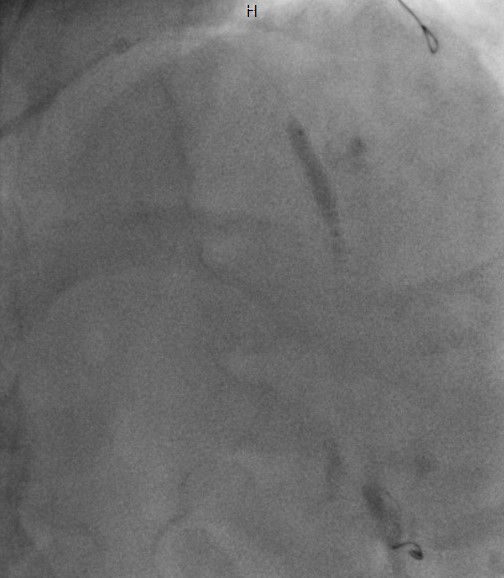
Through trans- radial approach, PCI of RCA lesion was done with a DES, 3.25x23mm Xience Alpine after pre-dilatation. Postdilated with 3.5x12mm NC balloon at 18atm with good final result. LAD lesion looked simple and straight forward and hence stented directly with one DES,3.0x15mm Xience Alpine at 14atm.CAG showed under expansion of the distal half of stent due to calcium. Post-dilated with 3.5x12mm NC balloon at 18atm, but under expansion persisted.Then dilated further with OPN NC super high pressure balloon which was a new addition to our inventory. On hearing the RBP of the balloon as 35atm,the assisting operator mistook it for the inflation pressure recommended by the primary operator and inflated directly up to 35atm at first instance. Immediate angio showed perforation in mid stent with active jet extravasation into the pericardium(TypeIII). Perforation was immediately treated with a covered stent 3.5x19mm Graft master at 16atm and post dilated at 18atm. Check angio showed sealed perforation with no further leak. Echo showed mild pericardial effusion without tamponade. Patient was observed for half an hour in cath lab and then shifted to CCU. Serial Echo did not show any further pericardial effusion. Check CAG next day showed patent stent in LAD with mild slow flow.
   - Case Summary:
Coronary artery perforation is a rare and potentially lethal complication of PCI. Earlydetection and immediate management are of paramount importance and can reduce the mortality and morbidity. Exercise caution while dilating the coronary lesion and refrain from under estimating the complexity of the lesion.
|
|