Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191019_002
| CORONARY - Complications | |
| STEMI Due to Sub-Acute Stent Thrombosis | |
| Samrany San1, Sokha Chan1, Chour Sok1 | |
| Calmette Hospital, Cambodia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
P.P, male, 81 years-old
-Relevant clinical history and physical exam:
A 81 year-old male was admitted for acute severe chest pain, 7 hours after onset. He had a history of ex-smoking, hypertension, CKD and COPD/pulmonary tuberculosis. On arrival, he had cardiogenic shock (BP 55/23 mmHg, HR 42 bpm).Following admission, he experienced ventricular fibrillation, synchronized cardioversion 360 j was done 2 times. Intravenous of dobutamine, dopamine and adrenaline was initiated. The decision was taken to proceed immediately with coronary angiography.
-Relevant test results prior to catheterization:
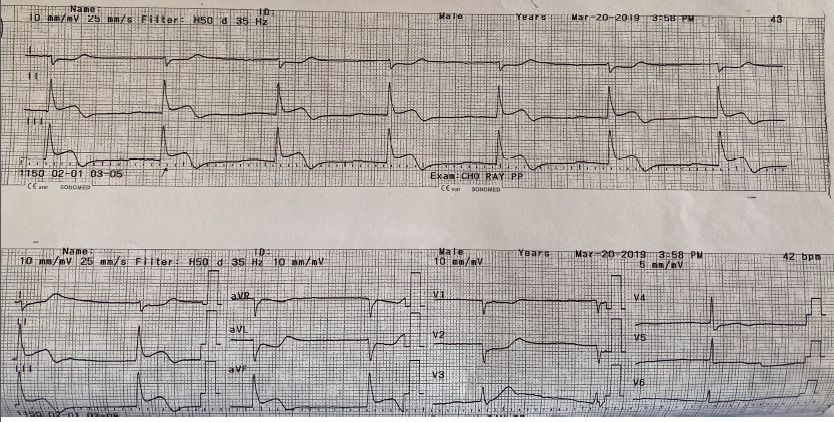
Electrocardiography (ECG) showed complete AV block, ST segment elevation in II, III, aVF, V3R and V4R(Fig 1.). Echocardiography revealed a severe systolic dysfunction (LVEF = 30%).
 - Relevant catheterization findings:
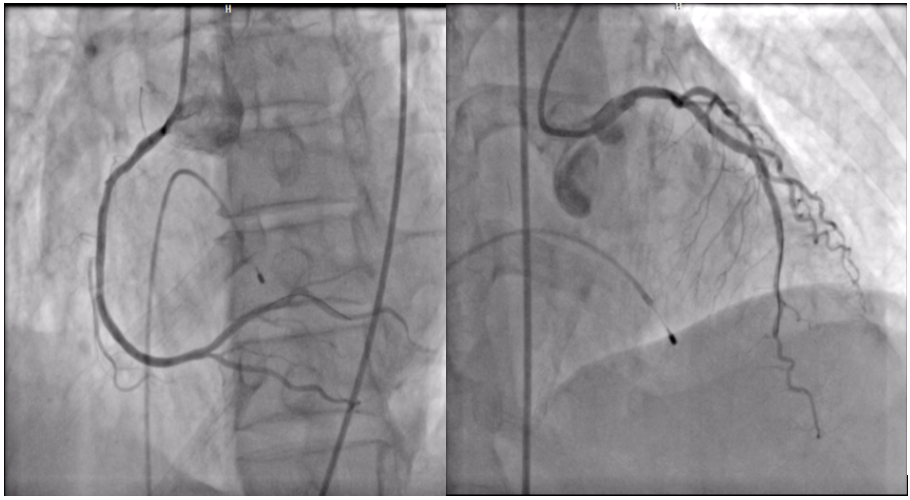
Left coronary angiography revealed severe stenosis mid LAD with TIMI 1 flow. (Video.1)Right coronary angiography demonstrated thrombotic occlusion mid RCA(Video.2).
|
|
|
[Interventional Management]
- Procedural step:
A 6F and 5F sheaths were inserted through right femoral artery and vein. Temporary pacing was placed. Due to cardiogenic shock, complete revascularization was performed. We deployed a Resolute 3.0mm x 38mm stent in the mid RCA as a culprit vessel, and Integrity 2.75mm x 30mm stent,Integrity 3.0mm x 22mm stent in the mid and proximal LAD after predilation by balloon Sprinter Legend 2.0mm x 20mm. Final angiography showed a good result with TIMI 3 flow (Fig. 2). The hospitalization was complicated by pneumonia and cardiogenic shock. On the thirteen day, he can discharged without any symptoms. Unfortunately, 15 days after discharged, he suddenly complained chest pain and ECG changed (ST elevation in DII, DIII, aVF). Emergent coronary angiography showed thrombotic total occlusion in the RCA, which represented subacute stent thrombosis (Video 3). We did the thrombus aspiration of RCA with Export catheter for twice times and a few grow clots were sucked out. Cause of appeared hazy in the stent, 2 Resolute 3.0mm x 30mm stent and 3.0mm x 38mm stent were deployed in the mid and proximal RCA. Post-dilatation performed with NC Sprinter Legend balloon 3.5mm x 15mm to intend well expanded stent. Final angiography showed TIMI 3 flow in the RCA (Video 4). After detail explore the cause, he declared self-interrupt taking antiplatelet in 5 days before the event. Finally the patient was discharged with medication in 7 days later. 6 months follow-up, he has no clinical symptoms.
 - Case Summary:
Subacute stent thrombosis is commonly to present with STEMI and cardiogenic shock leading to fatal threaten, Emergent treatment is mandatory. In our case, premature self-discontinue antiplatelet was the most likely cause of the stent thrombosis. The multi-modality imaging such as IVUS and OCT would help us to confer significant information and discover the exact etiology (underexpansion,edge dissection, stent fracture or malapposition).
|
|