Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20190831_006
| CORONARY - Complications | |
| Disasters Come One After Another. | |
| Ta-Hsin Tai1, Feng Yu Kuo2, Wei-Chun Huang2, Guang-Yuan Mar2 | |
| Kaohsiung Municipal United Hospital, Taiwan1, Kaohsiung Veterans General Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Huang
-Relevant clinical history and physical exam:
The patirnt has history of coronary artery disease with triple vessels disease in NSTEMI s/p PCI few months ago. He came to our ward for stage PCI this time. No chest tightness or other discomfort was mentioned since last hospitalization.
-Relevant test results prior to catheterization:
Previous vessels with stenting were in stable condition. No restenosis was noted. And RCA distal part with 70% stenosis was noted.
- Relevant catheterization findings:
We decided to treat RCA distal part. However, the catheter was poor support due to bending subclavian artery. We could not pass our stent further. Guldeliner was used for better support. But stent dislodge occurred. We switched to femoral artery approach. Then disasters come one after another. Right femoral artery dissection wsa noted .
|
|
|
[Interventional Management]
- Procedural step:
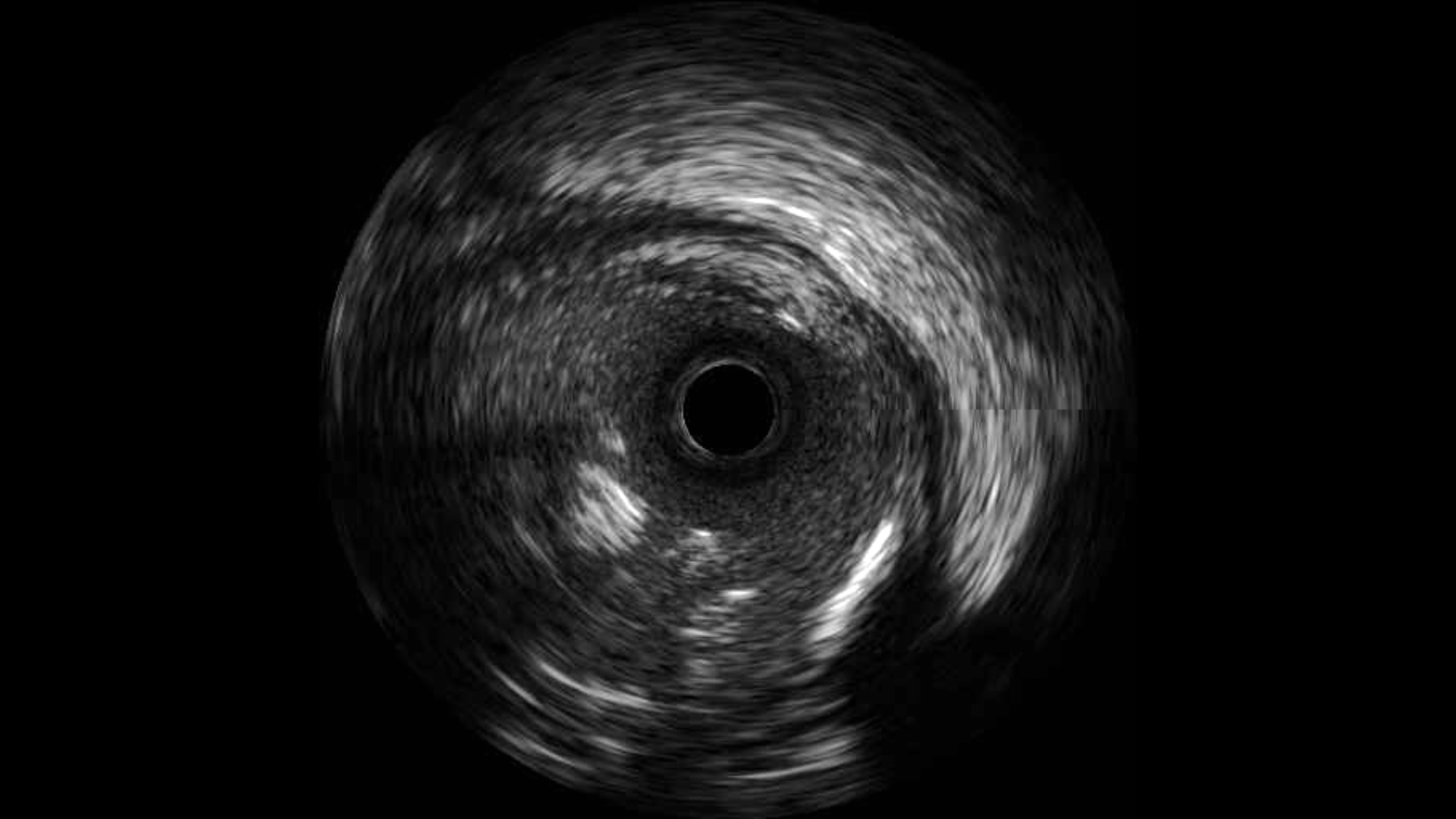
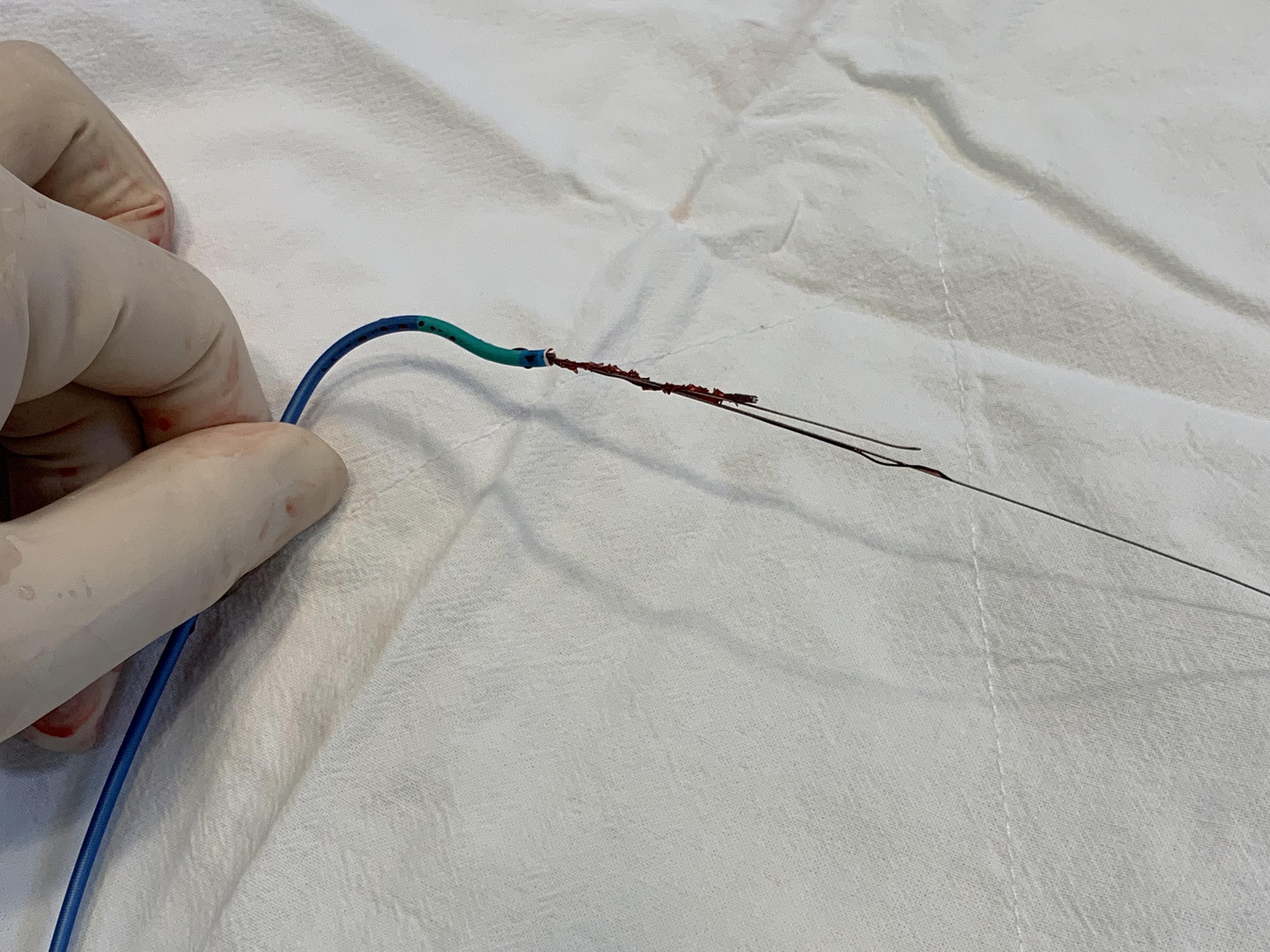
Finally, we have good support from left femoral artery approach. We passed one wire to across the stent. Then IVUS was performed. We could see the proximal part of stent was partial depolyed. The distal part of stent was in RV branch. We passed two more wire to across the stent. Then twist all wires together. Pulled out the stent with the whole system. No perforation or vessels jailed was noted. After gulideliner support, we completed the whole PCI with one DES over RCA distal lesion. We left the right femoral artery dissection due to no pressure damping or other progression.
  - Case Summary:
Both stent dislodge and iatrognic peripheral artery dissection were disasters in PCI. Always check up the stent every time if the delivery was failed. There were several technique to remove the dislodge stent . Twisted wire technique was a safe and efficacy way. We did not treat the right formal artery dissection due to no pressure gradient. No bruit after the whole procedure.
|
|