Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20191103_0001
| Bifurcation/Left Main Diseases and Intervention | |
| First Experience of Complex Bifurcation Lesion Treatment with Contemporary Implantation of Two Different Bifurcation Dedicated Stents: First for Side Branch Scaffolding and Second for Main Branch Stenting | |
| Farhat Fouladvand1, Sashko Zhezhovski2, Oktaj Maksudov2, Dimitar Mitzov2, Yanko Cherkezov2 | |
| Clinica San Carlo, Italy1, Bulgarian Cardiac Institute, Bulgaria2 | |
|
Background:
Treatment of the through bifurcations is often challenging procedure requiring operator experience and excessive contrast and X-ray time. Though provisional stenting is preferred strategy not rarely two stents strategy is needed. Standard stents are designed to treat straight segments and not bifurcations where excessive strut deformation is needed. Dedicated stents can offer better behaviour it the bifurcation side and are divided in two major categories: those to treat the main branch (MBS) and those that protect the side branch (SBS). Bioss LIM (Balton, Poland) is main branch dedicated stent eluting Sirolimus and respecting the fractal geometry of the bifurcation with larger in diameter proximal part than the distal one. Two connecting struts join both proximal and distal parts that are mounted on specially designed tapered balloon. Advantage of this stent is very easy access to the side branch. Available dedicated stents that scaffold the side branch are Tryton (Tryton Medical, Durham, UK) bare metal stent and recently developed BioMime Branch (Meril, India) Sirolimus eluting stent. Distinguish characteristic of both stents is scaffolding of the side branch, presence of transition zone at the level of the carina and proximal main branch part being just anchoring the system to the vessel. Both stents require finalizing of the procedure by implantation on the main vessel of standard drug eluting stent. We decide to adopt both type of dedicated stent for through bifurcations (fig.1.) as first to implant the dedicated side branch stent (Tryton or BioMime Branch) and after that to fix the main branch with second dedicated stent Bioss Lim. By this technique we tried to have less metal at the carina side but to have easy access to the side branch for kissing balloon.
|
|
|
Methods:
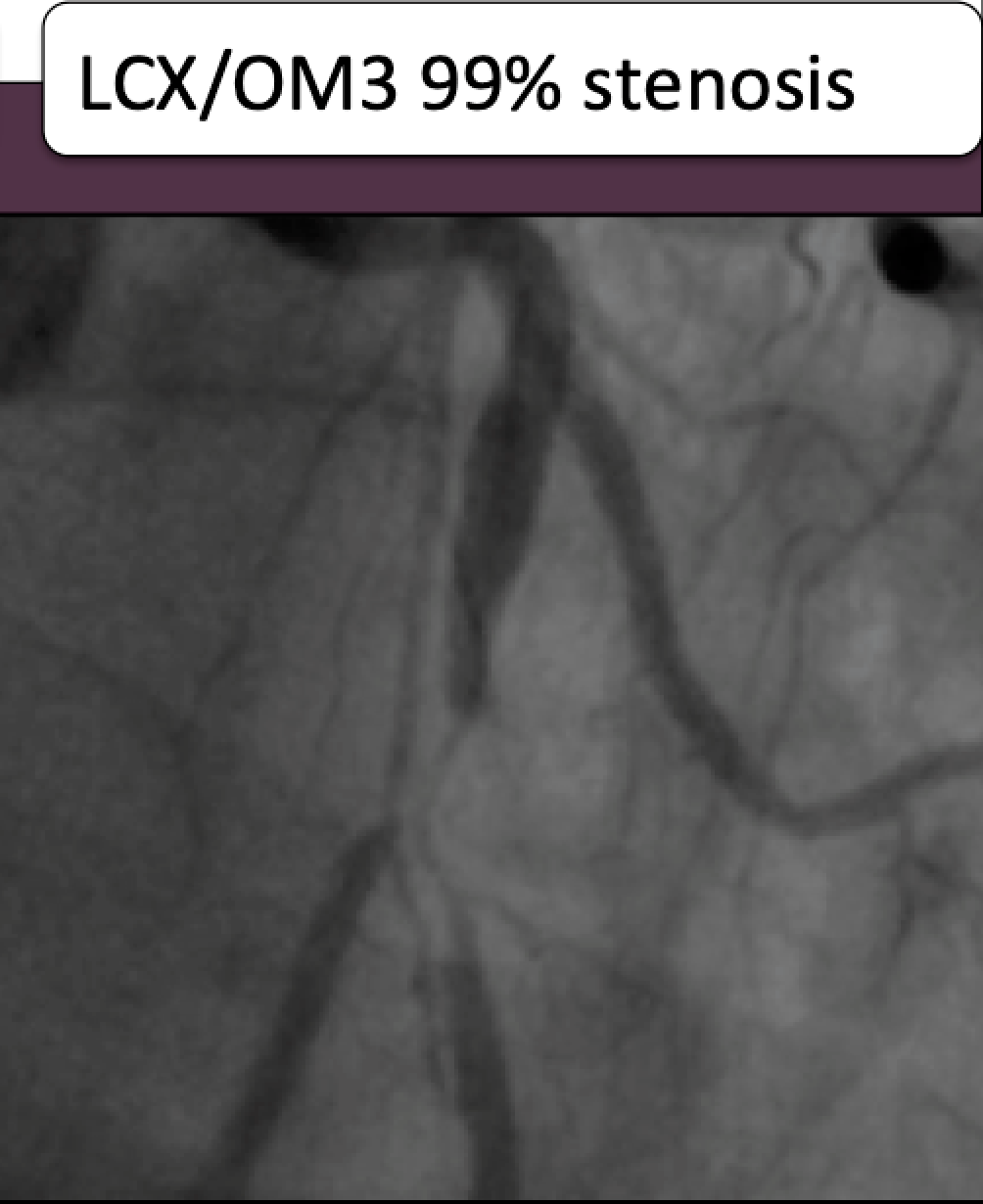
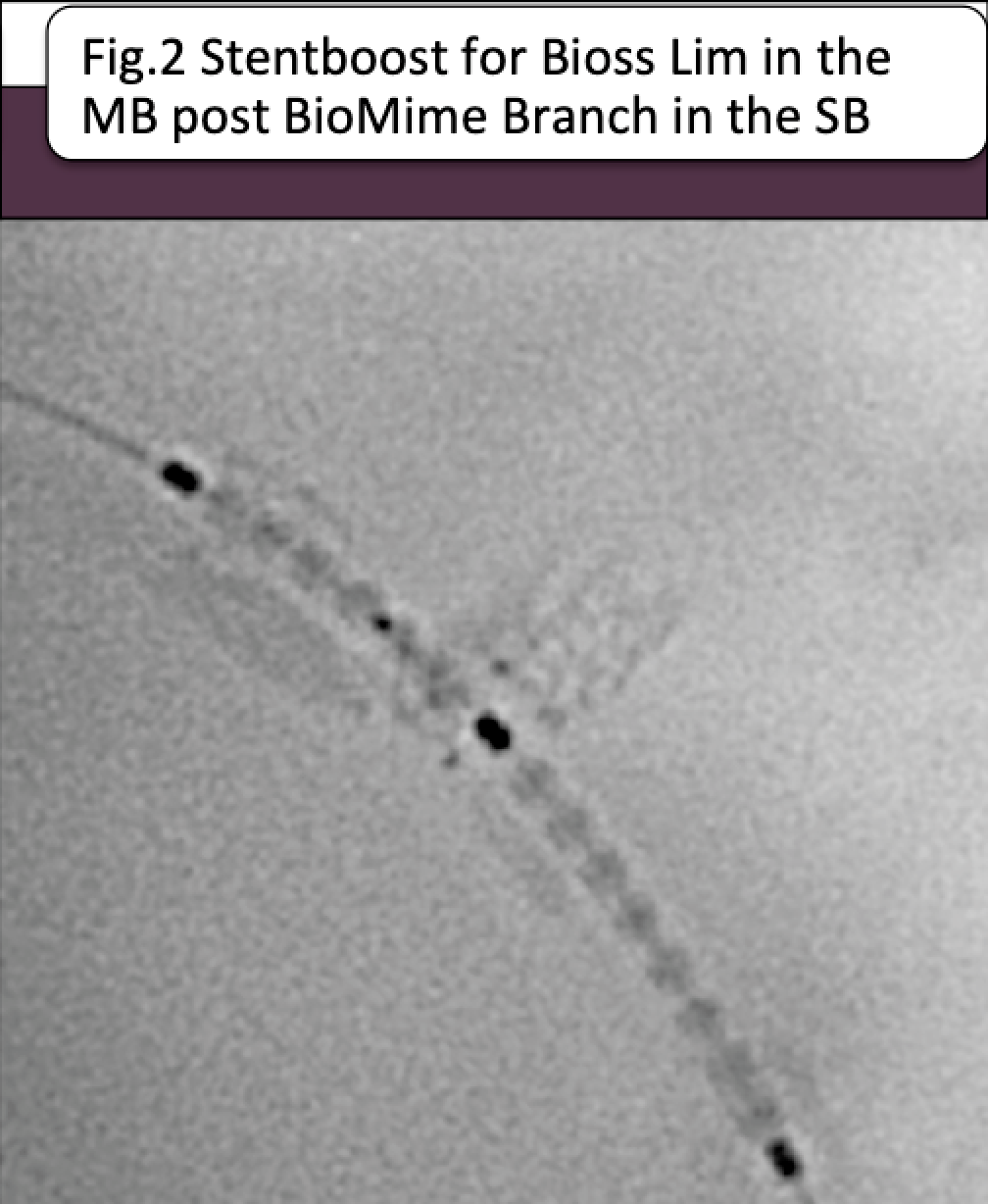
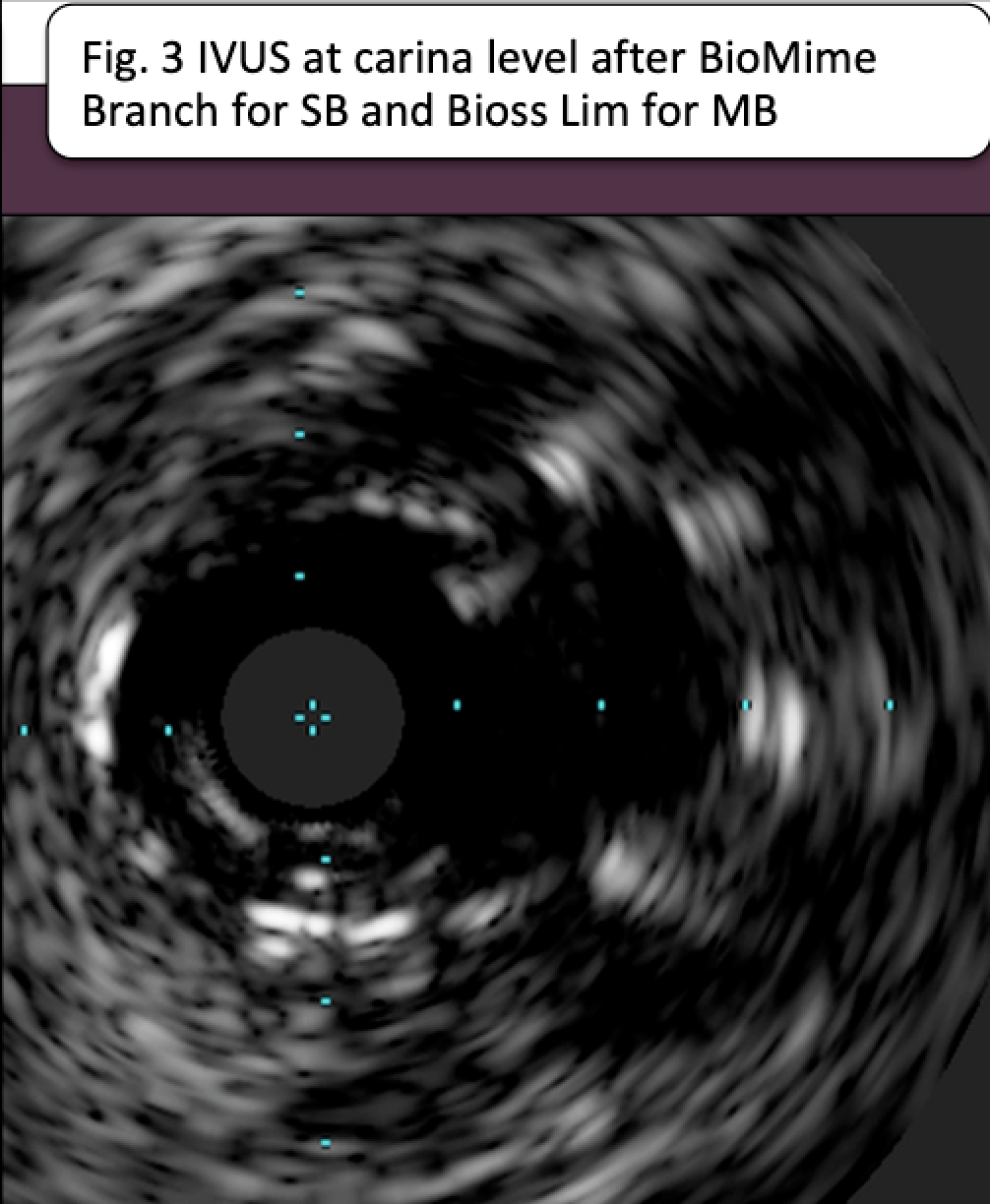
From Jan 2018 to August 2019 we treated 14 pts with coronary bifurcation. Mean age 65±12y from them 11 were males. All lesions were Medina 1.1.1. and by initial decision the strategy was to use two stents. The distribution was 12 LAD/D1 and 2 LCx/OM1 bifurcations. Mean MB diameter was 3,2±0,7mm, mean SB diameter was 2,7±0,5mm, mean MB stenosis length was 19,3±1,3mm and the length for SB stenosis was 3,3±0,7mm. Mean stenosis for the MB was 82±13,5%. Stable angina was seen in 11 of patients and ACS in the rest three. In 9 patients IVUS was used as adjunctive diagnostic method at least at the end of the procedure and in 5 patients catheter based FFR was used during and the end of the procedure. In 9 patients the SB was treated with Tryton stent with mandatory post-dilatation with drug coated balloon. In the remaining 5 patients the SB was treated with BioMime Branch DES. Briefly describing the procedure in all patients predilatation of both branches was performed and also kissing balloon dilatation was done before SB stent placement. Once the SB stent was positioned controlling in two angiographic projections a POT with 0,5 mm larger balloon was performed. Keeping the balloon within the proximal part of the stent, the wire from SB was repositioned in the MB. Then a second dedicated DES - Bioss Lim was positioned in the main vessel. The precise position was confirmed using Stent boost (Fig.2). After second stent deployment a second POT was performed in all cases. After that rewiring of the SB was done and the procedure was completed by second kissing balloon dilatation (in case of Tryton stent performed with drug coated balloon toward the SB) and final POT. Mandatory the procedure was ended either by IVUS study (Fig.3) or FFR measurement (Fig.4). Variable as wire, balloons and contrast use as also procedure time and X-ray time as also procedure and device success were calculated. One and six months clinical follow up were planned as also angiographic control at one year.
  |
|
|
Results:
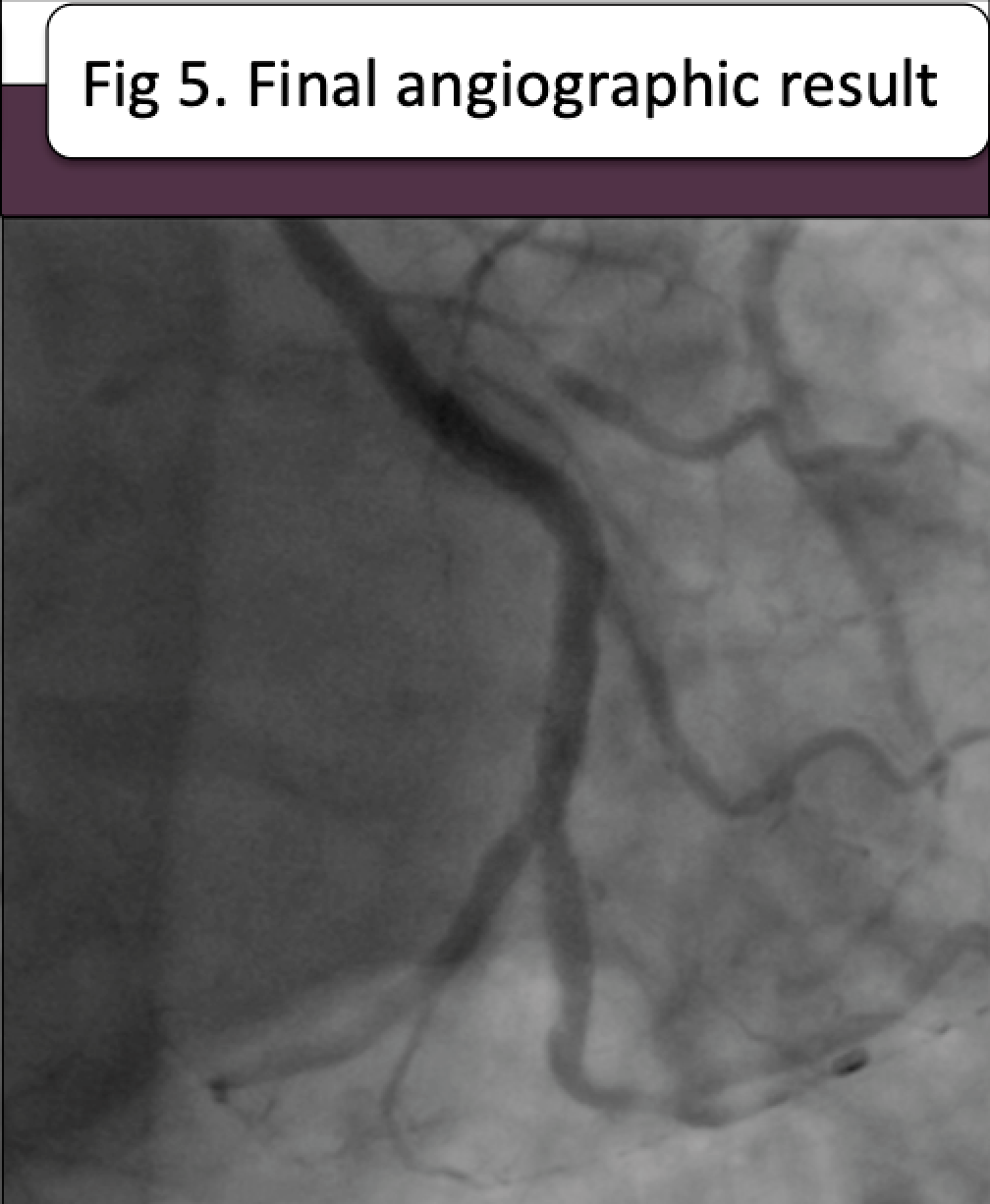
Radial approach was used in all patients. Mean procedure time was 129,8±19,9 min and the mean X-ray time was 28,8±7,0 min. Mean amount of contrast dial was 104,9±22,6 ml. Mean number of coronary wires was 2,4±0,6; mean number of all type balloons was 5,7 ±1,2. Procedure success was achieved in all patients and device success (Fig. 5) for both stents was also 100 percent. We were able to position all side branch dedicated stents at first attempt. Repositioning of the wire from SB toward the MB didn't present any difficulties. All second dedicated stents Bioss Lim without the need of further predilatation passed and were implanted with success. To mention the better visualization of the BioMime Branch stent respect the Tryton stent. Also to mention the relatively higher cost of the procedure performed with Tryton stent as the balloon for the SB during the final kissing was drug coated one with the idea to reduce the rate of SB restenosis as the Tryton stent is bare metal. Should be emphasised that the re-crossing with wire and subsequently with balloon through the struts of Bioss stent toward the already scaffold SB was relatively easy and in all cases with success. In all 5 patients where at the end we performed FFR measurement the MB FFR was > 0,94 and the SB FFR was also > 0,92. In the 9 patients where we performed final IVUS assessment the probe easily passed in both MB and SB and the carina was well opened as also the both stents were well apposed to the vessel wall. All patients at first month follow up were free of symptoms. Up to the moment 4 patients were studied at one-year follow-up and the angiographic result demonstrated luck of restenosis of both BM and SB in all of them.
 |
|
|
Conclusion:
The bifurcation dedicated stents in some favor anatomic situation are adjunctive devices that can facilitate the success of the procedure. Both dedicated stents used in our work either MB dedicated one Bioss Lim either SB scaffolding stent Tryton and BioMime Branch demonstrate easy placement particularly when all steps of bifurcation treatment procedure are respected. Bioss Lim DES due to its design has the advantage to permit wide access toward the SB, particularly when the SB is already stented. Tryton stent being BMS could be associated in relatively higher probability of SB restenosis that could be overcome by adopting the post-dilatation with drug coated balloon but evidently for higher procedure cost. The new dedicated bifurcation stent BioMime Branch benefit the presence of drug Sirolimus and by this can be used even in diabetic patients and probably at low restenosis rate. The combination of dedicated side branch stent especially if it is drug eluting and there after placing a dedicated MB stent has the rationality to reduce the amount of metal at the carina site and to permit SB access during the procedure. This combination according to our experience is absolutely feasible and without increasing the procedural risk of complication as also without increasing the procedural variables as time and contrast amount.
|
|