Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
ABS20191101_0009
| Valvular Intervention: Aortic | |
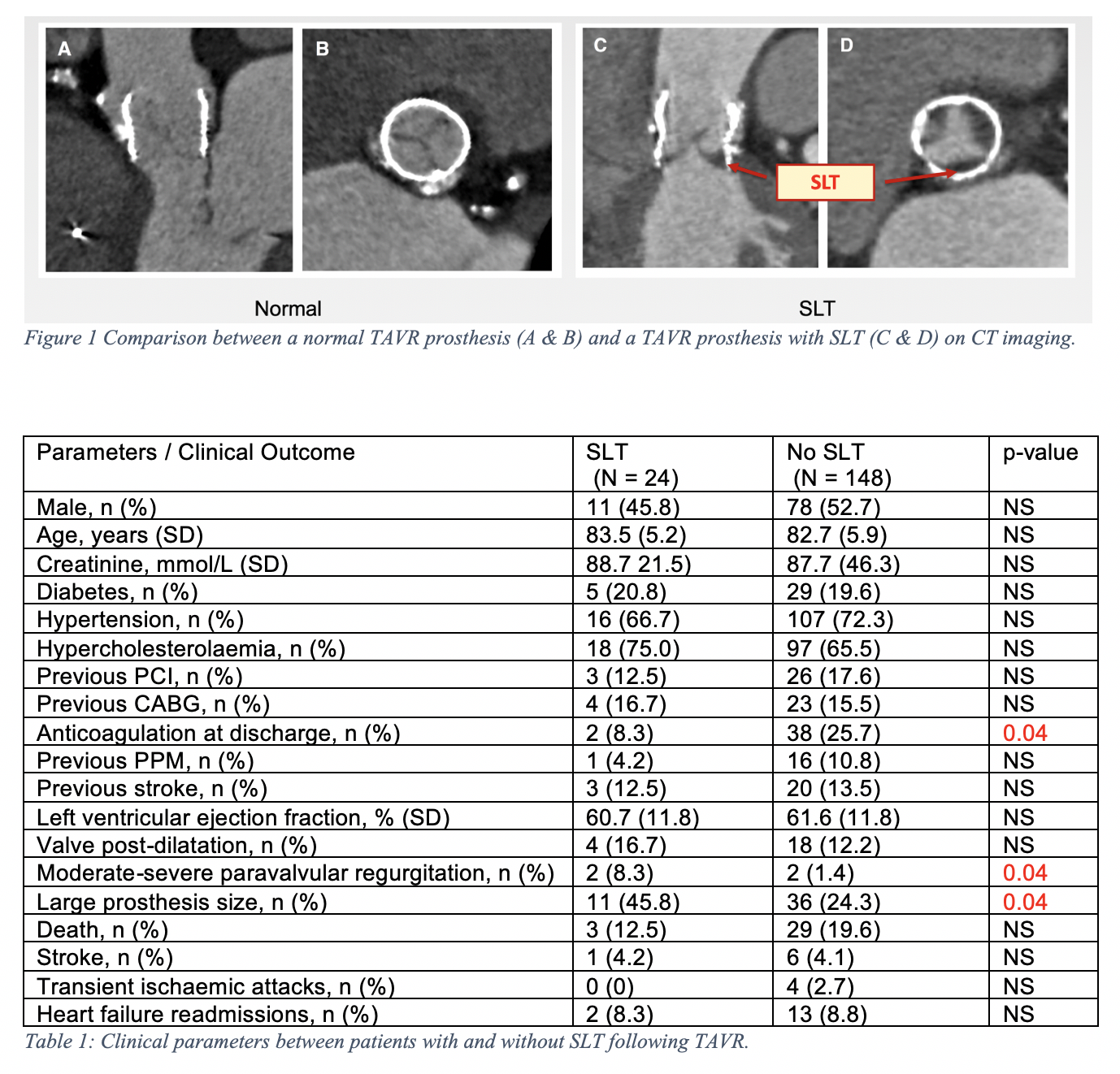
| Clinical Predictors and Impact of Leaflet Thrombosis Following TAVI with 320-Multislice CT at Medium Term Follow-Up | |
| Hashrul Rashid1, Nancy Khav2, Sean Tan2, Arthur Nasis3, James Cameron3, Rob Gooley3 | |
| Monash University, Australia1, Monash Health and Monash University, Australia2, MonashHeart and Victorian Heart Institute, Australia3 | |
|
Background:
Computed tomography (CT) defined subclinical leaflet thrombosis (SLT) following transcatheter aortic valve implantation (TAVI) has recently been described. There is limited data on this condition.
|
|
|
Methods:
Patients were evaluated prospectively with CT following TAVI. All examinations were performed with a 320-multislice CT (Aquilion One, Canon) with ECG-gated acquisition. Images were assessed on a dedicated workstation (3Mensio, Pie Medical Imaging) with multiplanar reconstruction for presence of SLT, defined as hypo-attenuating leaflet thickening. No patients had clinical leaflet thrombosis (overt heart failure with high prosthesis gradients).
|
|
|
Results:
172 patients [89 (51.7%) male, mean age 82.8±5.7 years, STS score 5.1±2.1%] were included in this analysis [Lotus valve 54%, Core valve 32% and Sapien valve 14%], with median CT-scan of 6 weeks post TAVI. Characteristics and potential associates of SLT are shown in the table. The overall prevalence of SLT was 14% (24 cases) with a trend towards lower rates of SLT with Core valve (7.3%), in comparison to Lotus (17.2%) and Sapien valves (16.7%) (p = 0.07). Patients who developed SLT were less likely to be on anticoagulation at discharge (8.3% vs 25.7%, p = 0.04), received larger TAVI prostheses (45.8% vs 24.3%, p = 0.04) and higher rates of moderate-severe paravalvular regurgitation (PVR) with SLT (8.3% vs 1.4%, p = 0.04). There no difference in the rates of death, stroke or transient ischemic attacks at median follow-up of 2 years.
 |
|
|
Conclusion:
Absence of anticoagulation, large TAVI prosthesis and moderate-severe PVR were predictors of SLT. There was a trend towards lower rates of SLT with Core valve. SLT did not lead to increased adverse outcome. Further studies are warranted to determine the long-term impact of SLT following TAVI.
|
|