
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-173
Drug Coated Balloon in Chronic Total Occlusion - PCI, New Hope in Coronary Intervention
By Taslima Afroz
Presenter
Taslima Afroz
Authors
Taslima Afroz1
Affiliation
United Hospital Limited, Bangladesh1,
View Study Report
TCTAP C-173
Coronary - DES/BRS/DCB
Drug Coated Balloon in Chronic Total Occlusion - PCI, New Hope in Coronary Intervention
Taslima Afroz1
United Hospital Limited, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 67 years old, male, diabetic, hypertensive, presented with severe central chest pain for two days. Exertional chest pain for last one year. Hs Troponin I was raised, ECG showed anterior ischemia. He has H/O PCI to LAD in 2012 and re-look CAG in 2021. Re-look CAG showed 30 -40% ISR in proximal LAD. LCX and RCA were normal. On examination his vitals were with in normal limit and systemic examination revealed nothing significant.
 DCB in CTO-PCI.zip
DCB in CTO-PCI.zip
Relevant Test Results Prior to Catheterization
Hs Troponin I was raised (20,900 pg/ml)ECG showed anterior ischemiaEchocardiography showed anterior ischemia with fair LV systolic function Serum creatinine was 1.23 mg/dl, eGFR was 57ml/min.CAG revealed 100% ISR in LAD proximal and 60 to 70% de-novo lesion in OM, RCA was normal.
DCB in CTO-PCI.zip
Relevant Catheterization Findings
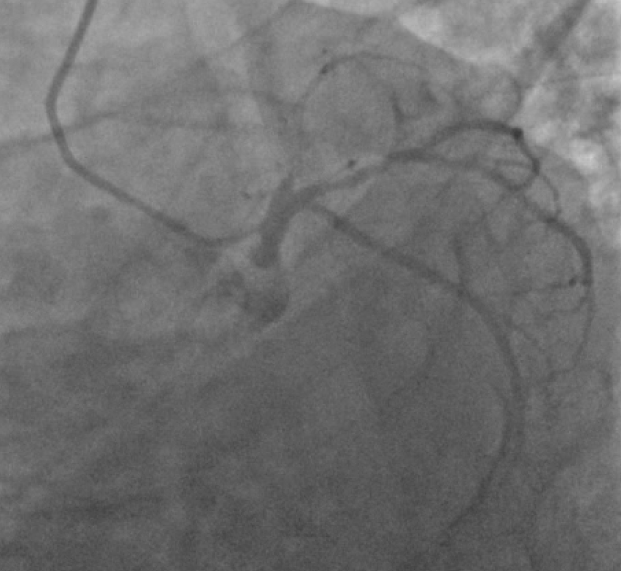
Coronary angiogram revealed 100% occlusion in proximal LAD stent which was 30 to 40% ISR in 2021, getting retrograde filling from right system and ipsilateral collateral. LCX was good size vessel having 60 to 70% osteo-proximal stenosis in the early origin of principal OM. RCA was dominant good size vessel and free of disease.
DCB in CTO-PCI.zip
Interventional Management
Procedural Step
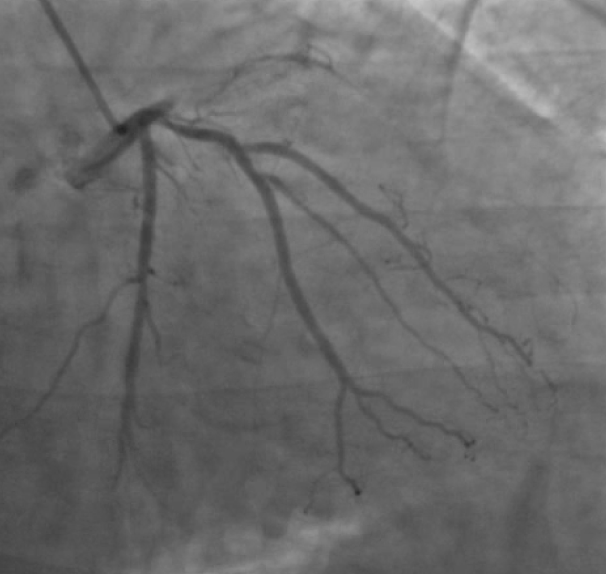
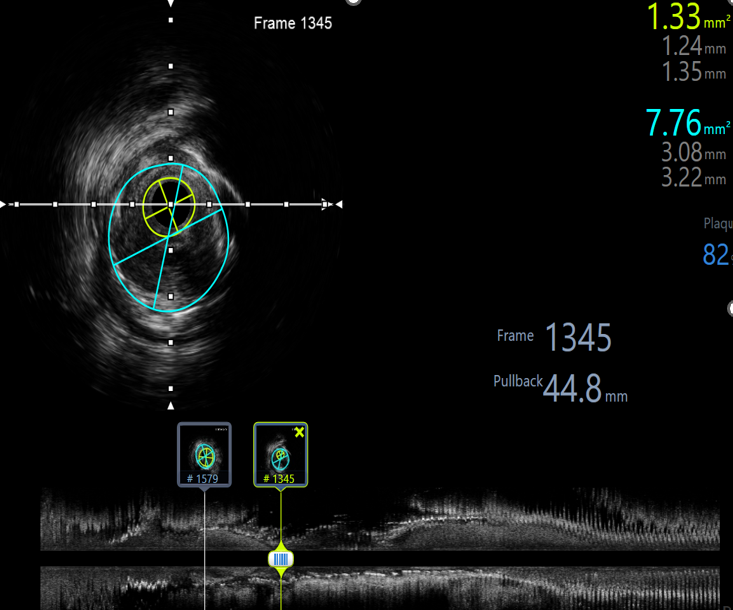
We decided to intervene LAD first and wiring it with Fielder-XT with the micro-catheter (Caravel) support. Sequential Balloon dilatation by 2X15 and 2.5X20 NC balloon at 14 ATM. Then IVUS was done in LAD and LCX. IVUS showed 1.33 mm MLA in the critical ISR in LAD proximal. Wire de-escalation with BMW wire and predilatation with 3X15 NC balloon at 14 ATM. A 3.5X25 mm DCB was inflated at 14 ATM for 1 mins, 2 times. IVUS was done in LAD which revealed 7.54 mm MSA, no dissection . IVUS pull back in OM showed 2.7 mm MLA in the osteo-proximal part. A 3.0X 16 mm DES was deployed and post dilatation was done by 3.5X15 mm NC balloon at 14 ATM. IVUS run in OM showed 7.41 mm MSA, well apposed stent. Final angiogram showed excellent post procedural result with good distal flow.
DCB in CTO-PCI.zip
Case Summary
DCB should be considered for the treatment of the CTO-ISR because the favorable result were obtained without an additional metal layer in addition with late luminal gain. We know that technologies are evolving for our patients comfort and operators should take their advantages for better clinical outcomes.