Coronary - Complex PCI - CTO
Successful Rotational Atherectomy After Invalid Intravascular Lithotripsy for Under-Expanded Old Stent Which Caused In-Stent Occlusion
Tetsuya Takahashi1, Taiga Ishigaki1, Tamon Yamanaka1
Japanese Red Cross Ishinomaki Hospital, Japan1,
A54-year-old man was performed percutaneous coronary intervention (PCI) for RCA twotimes at the age of 40 and 46 due to chronic coronary syndrome. He was admittedfor non-ST-segment elevation myocardial infarction, and primary PCI wasperformed for left circumflex coronary artery. Then, in-stent occlusion (ISO)of RCA was revealed.
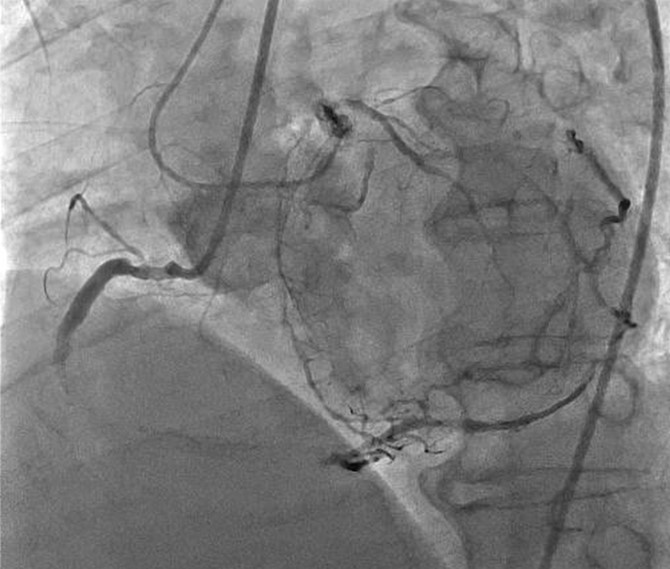
RCA ISOPCI was planned. The procedure was performed with an 8-Fr, JR 4.0 SH for the antegrade approach and a 5-Fr diagnostic catheter forretrograde angiography. Primary antegrade approachwas performed. Guidewire was successfully crossed to the distal true lumen by antegradewire escalation (XT-R knuckle into the ISO body, and Gaia Next2 puncture to thedistal cap).
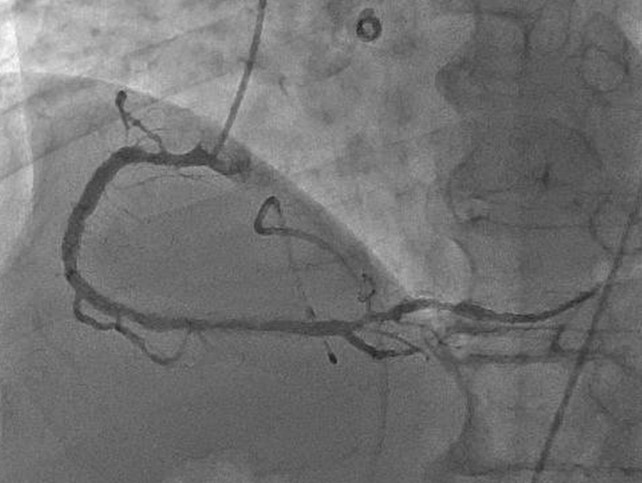
Intravascular ultrasound(IVUS) revealed an under-expanded old stent in the ISO mid lesion which mightbe the cause of ISO. Intravascular lithotripsy (IVL) was performed to the under-expandedstent. However, the stent expansion was not successful. Therefore, the PCIsession was finalized with drug coated balloon (DCB) to the ISO. Few monthslater, the 2
nd attempt PCI to the ISO was planned. Rotationalatherectomy (RA) with 2mm burr to the under-expanded stent was performed. Aftereffective RA, high pressure scoring balloon angioplasty succeeded stentexpansion, and DCB was used to finalize.

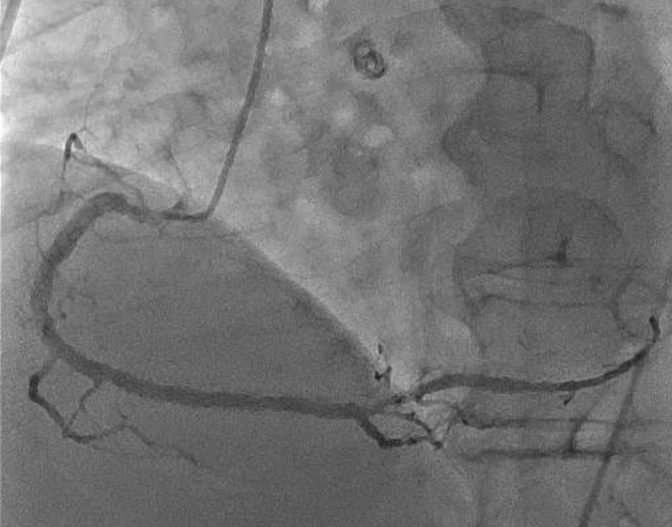
In stent restenosis and occlusion are big issues even in the current drugeluting stent era. In stent RA for under-expanded stent is complex and highrisk procedure. However, In stent RA for under-expanded stent is sometimeseffective strategy if IVL failed to expand stent.
