
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-088
Only Light Can Penetrate: Use of Laser Atherectomy in Uncrossable CTO Lesion
By Sai Man Wong
Presenter
Sai Man Wong
Authors
Sai Man Wong1
Affiliation
Princess Margaret Hospital, Hong Kong, China1,
View Study Report
TCTAP C-088
Coronary - Complex PCI - CTO
Only Light Can Penetrate: Use of Laser Atherectomy in Uncrossable CTO Lesion
Sai Man Wong1
Princess Margaret Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 74 years old gentle, who enjoyed good past health, complains of progressive unstable angina for 2 weeks. He was admitted for severe unstable angina that radiate to left shoulder.
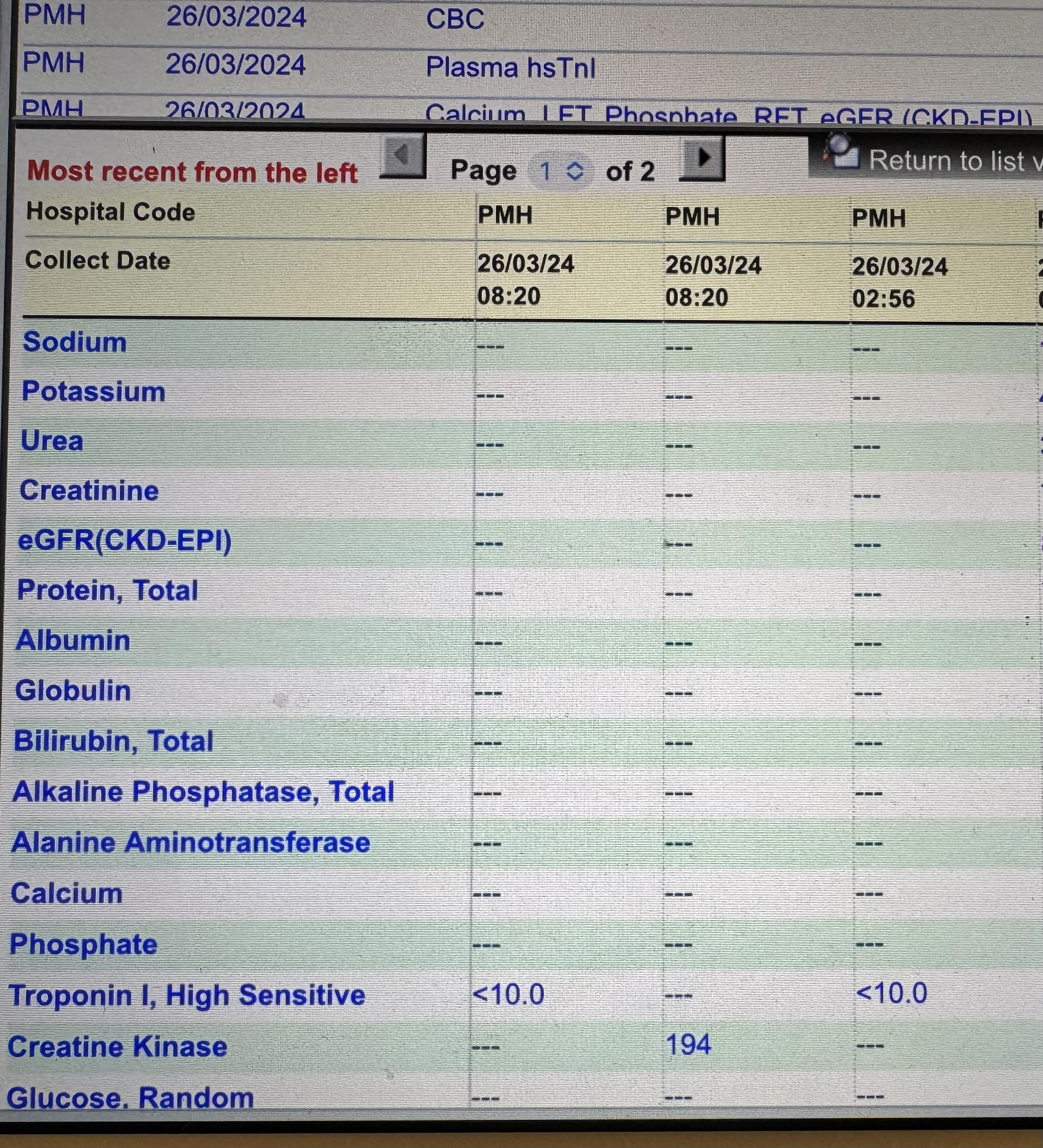
Physical examination was unremarkable. Serial troponin I was normal.
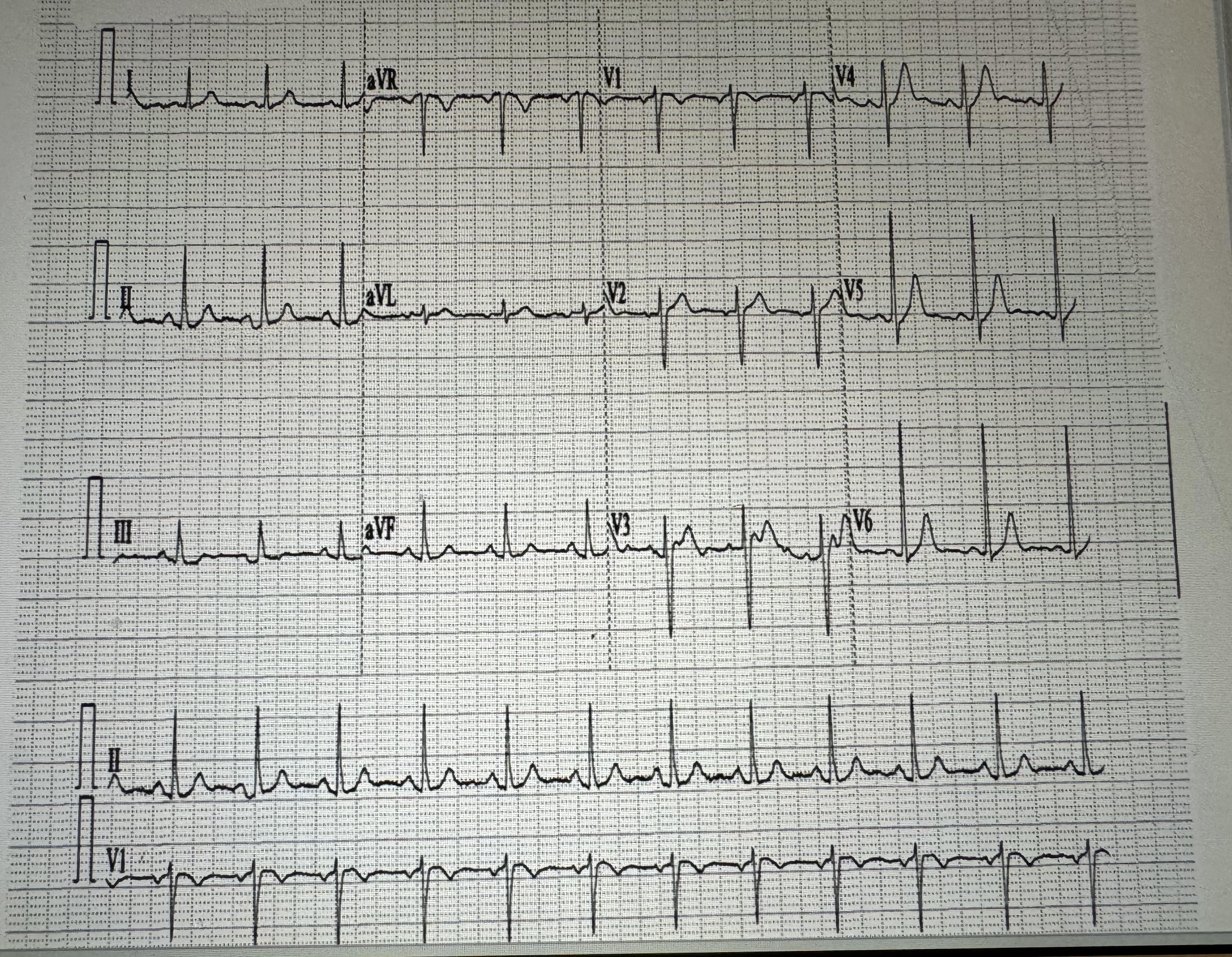
ECG showing sinus rhythm without acute ischemic changes.
Relevant Test Results Prior to Catheterization
private CT coronary angiogram was done:- Calcium score 1561- Severe stenosis at proximal RCA- Moderate stenosis at proximal LAD, D1, PLV- Mild stenosis over left main coronary artery, mid-LAD and sital LAD
Echocardiogram shows normal LV systoic function, no regional wall motion abnormality, valves unremarkable
Echocardiogram shows normal LV systoic function, no regional wall motion abnormality, valves unremarkable
Relevant Catheterization Findings
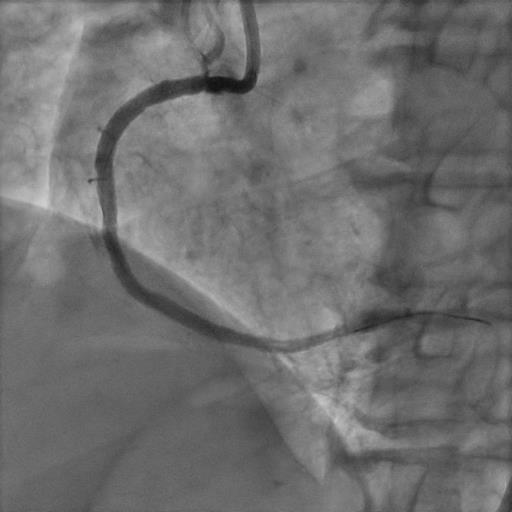
Coronary angiogram:LM mild diseaseproximal LAD calcified 80% stenosisLCX small and non-dominantpRCA CTO with collateral from LAD
Interventional Management
Procedural Step
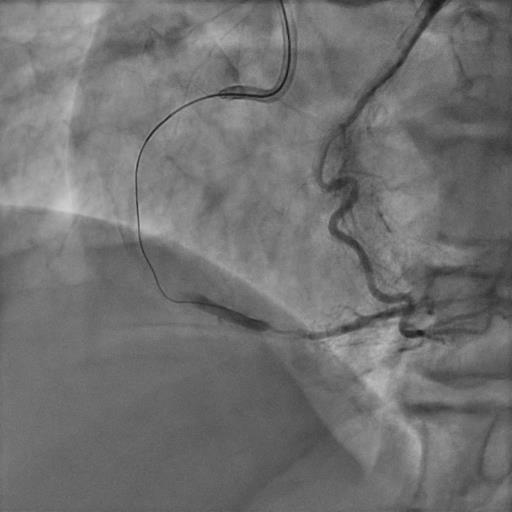
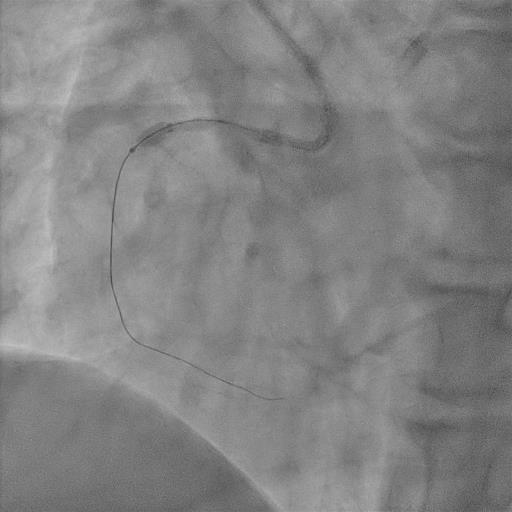
PCI was done to LM-LAD with DES 3.5 x 38, post dilated with 3.5 NC balloon. Fail to wire RCA in first procedure.Staged PCI to RCA was attempted. RCA was engaged with 8F AL 0.75 guiding. Attempted to wire RCA with Fielder XTA supported by Corsiar. Fielder XTA managed to went into distal RCA but suspected to go into subintimal space. Fail to advance microcatheter across CTO body thus fail to perform rotablation or orbectal atherectomy . Attempted 1.5/12 and 0.85/5 balloon but uncrossable. Excimer Laser Coronary Artherectomy(ELCA) remains the last resort for the uncrossable lesion.Laser artherectomy with contrast media was done to mRCA CTO body. Eventually able to pass 1.5/12 semi-compliance balloon and 2.5/10 cutting balloon for predilatation. IVUS catheter delievered successfully afterward to confirm guidewire position in true lumen distally. RCA was eventually stented with 3 DES balloon with good angiographical outcome.
Case Summary
We have demonstrated successful PCI to an uncrossable RCA CTO lesion with assist of Excimer Laser Coronary Artheretomy (ELCA). For the uncrossable lesion that neither microcather nor 0.85 balloon can be delievered, ELCA may be the last resort.