Structural - Surgical Therapy (Structural)
Recurrent Fresh Left Atrial Appendage Thrombus in Severe Rheumatic Mitral Stenosis: Transitioning Strategy for Optimal Management
Ingrid Maria Pardede1, Sunanto Ng1, Jessica Anastasia Setiawan1
Pelita Harapan University, Indonesia1,
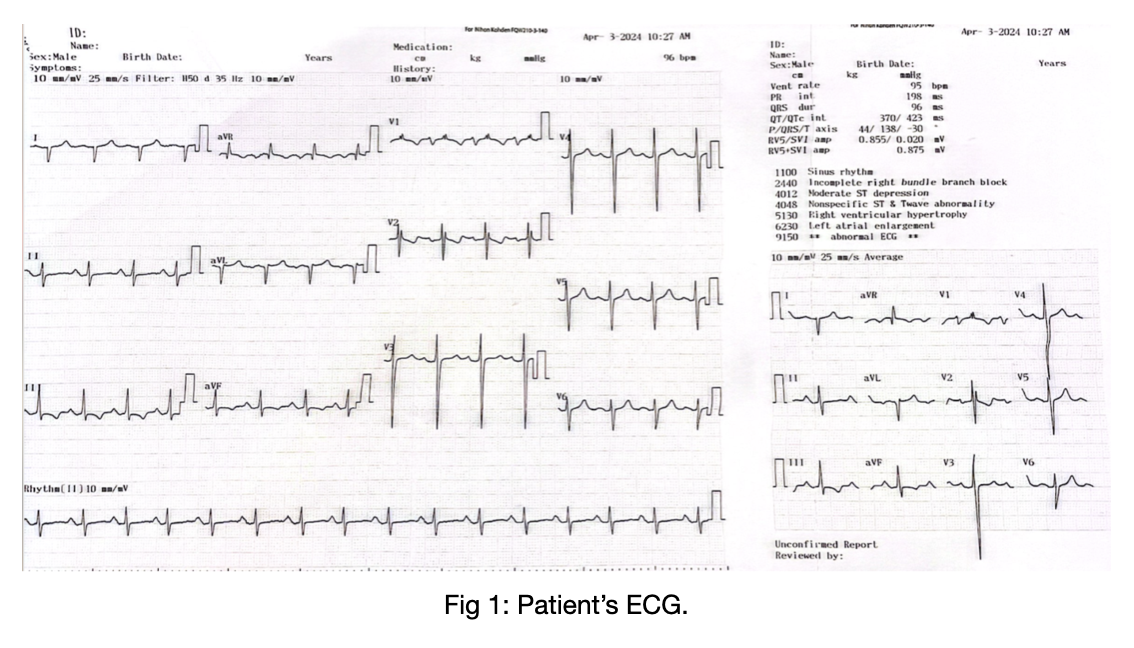
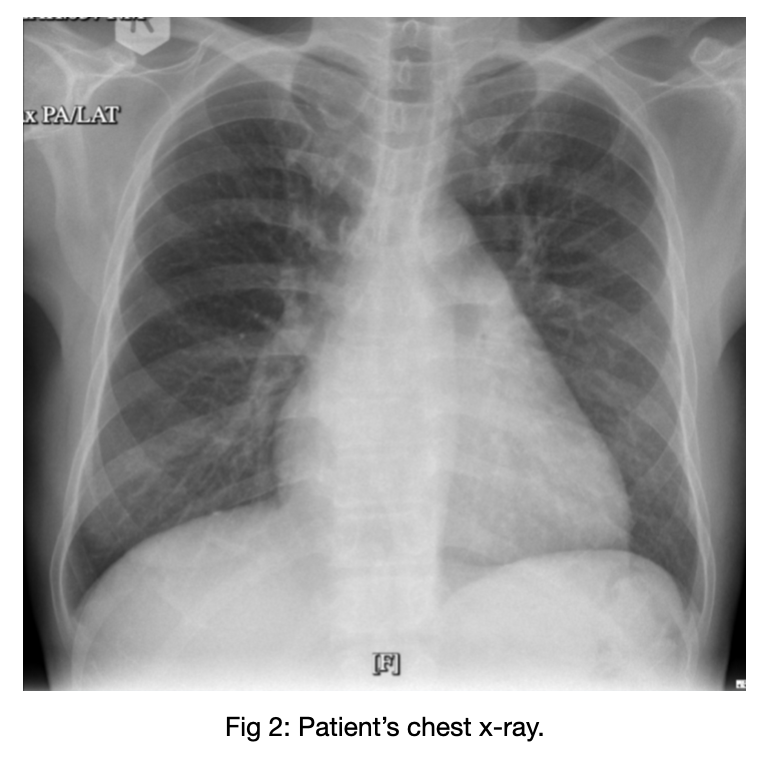
A 57-year-old male working as an aviation mechanic from Qatar came with worsening dyspnea on effort for 3 months with a previous history of uncontrolled DM (HbA1C 7.9 %). Physical examination was significant for diastolic murmur with opening snap, best heard at apex. ECG showed sinus rhythm, biatrial enlargement, RAD, RVH, incomplete RBBB. Chest x-ray revealed cardiomegaly with pulmonary artery dilatation and left atrial enlargement.
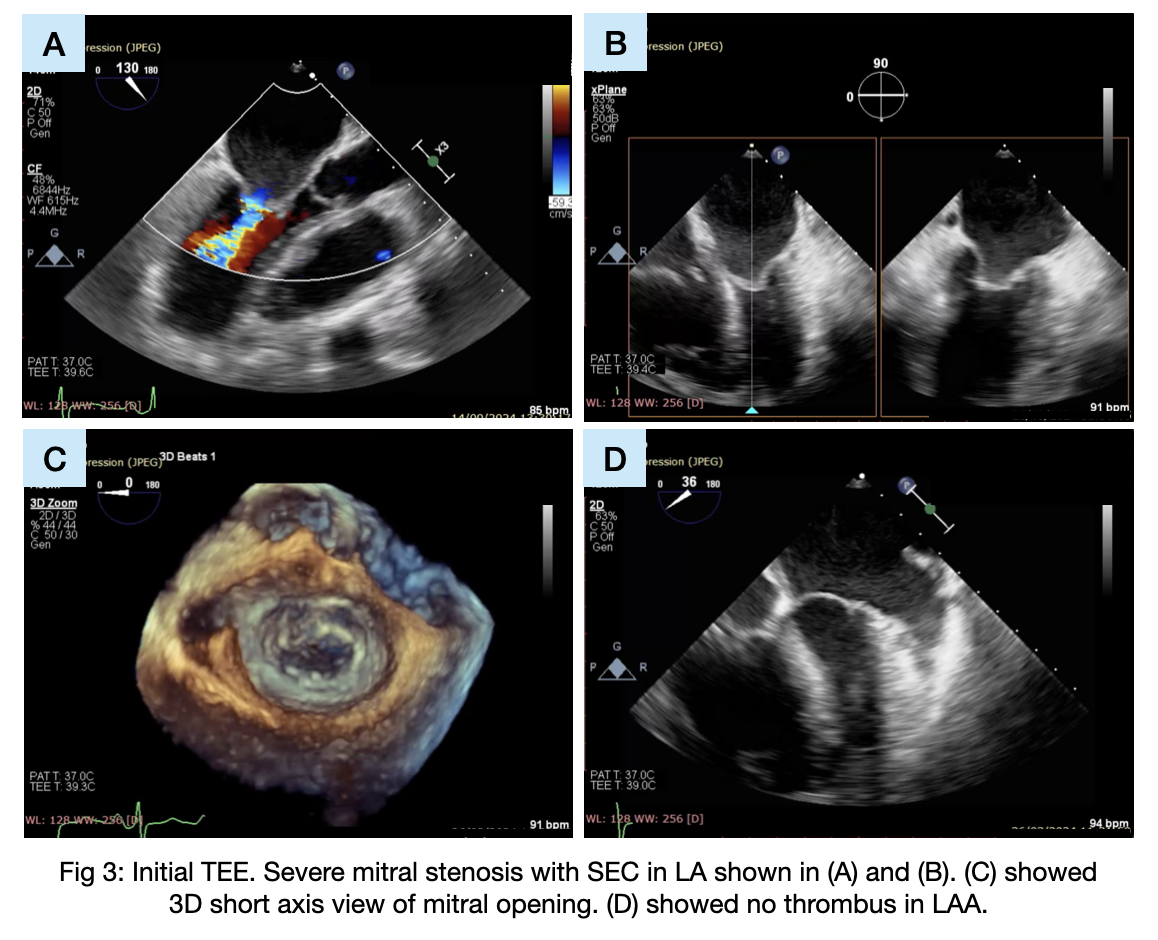
TEE showed severe mitral stenosis with rheumatic mitral morphology, MVA 0.6 cm2, mean/peak MVG 8/12 mmHg, Wilkins score of 8 favorable for BMV and pulmonary hypertension with secondary tricuspid regurgitation. In preparation for BMV, he was advised to consume warfarin for 3 months and achieved INR 3.5.
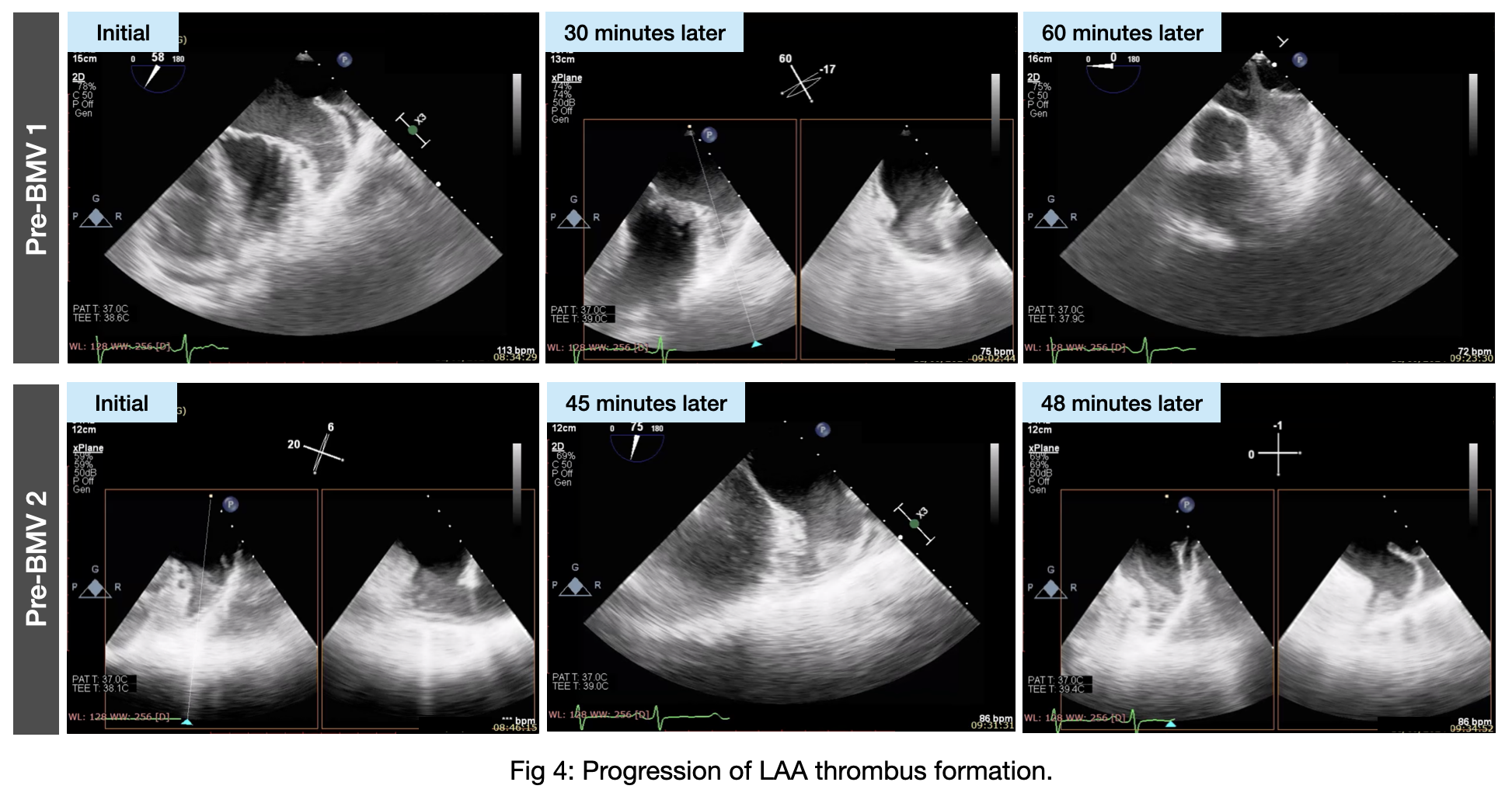
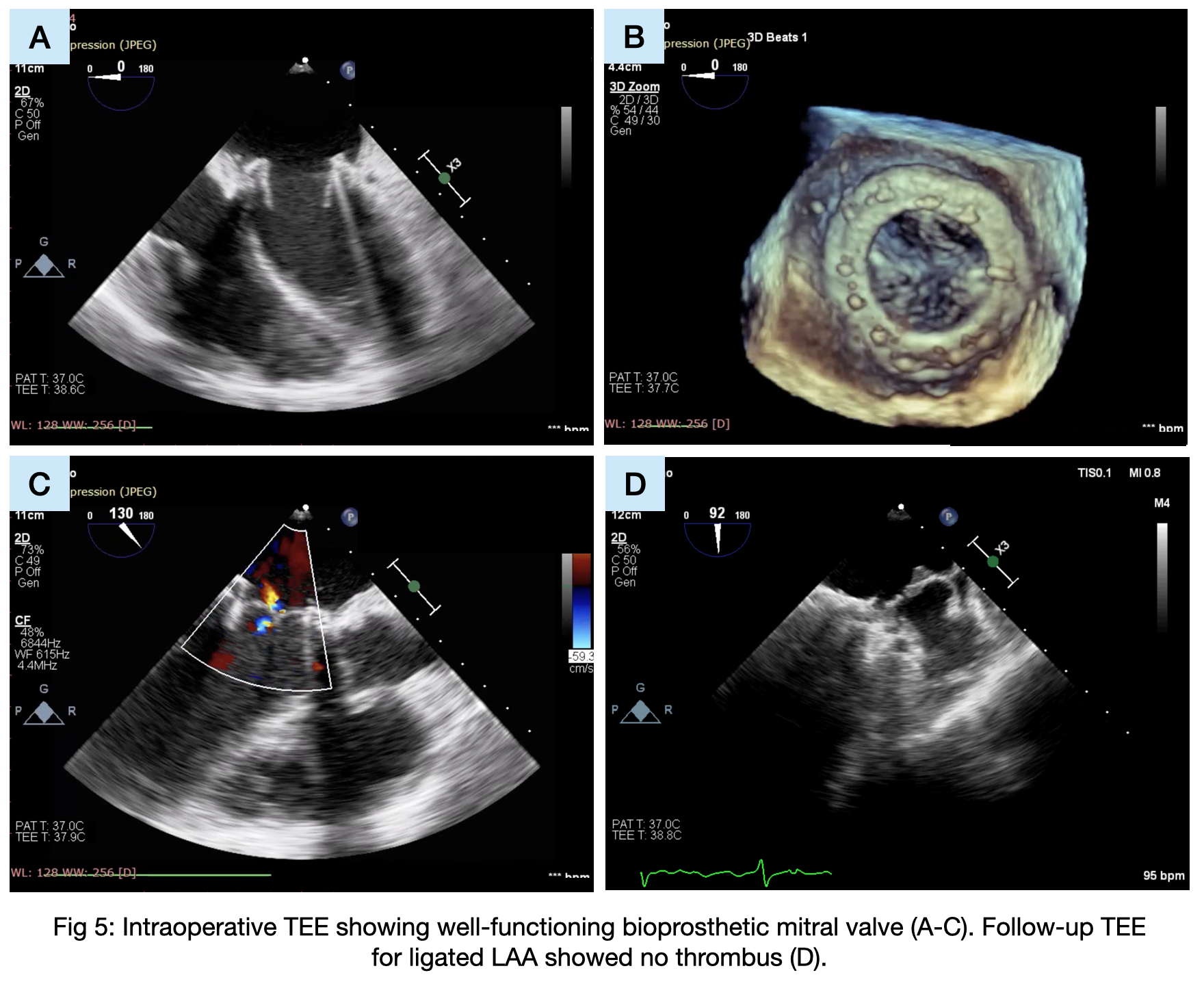
The initial plan for BMV was deferred twice due to thrombus recurrence, prompting a change in strategy to MVR with bioprosthetic valve and CABG for coexisting coronary artery disease. LAA plication effectively prevented further thrombus formation. Postoperative persistent atrial fibrillation necessitated rhythm control with electric cardioversion to restore sinus rhythm. Follow-up confirmed successful outcomes and maintained sinus rhythm, underscoring the importance of a multidisciplinary approach in complex cardiac cases.