TCTAP C-120
Coronary - Complex PCI - Long Lesion
Endless Loops: The Infinite Challenge of Complex RCA CTO Intervention
Kai Soon Liew1, Huan Yean Kang1, Chai Yih Tan1, Virginia Nancy1, Kay Leong Kenneth Khoo1, Subramaniam Prabahkar1, Mohd Khairi Othman1, Narasamuloo Kantha Rao1, Krishinan Saravanan1, Chee Tat Liew2, Karthikesan Dharmaraj1
Hospital Sultanah Bahiyah, Malaysia1, Penang Pantai Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
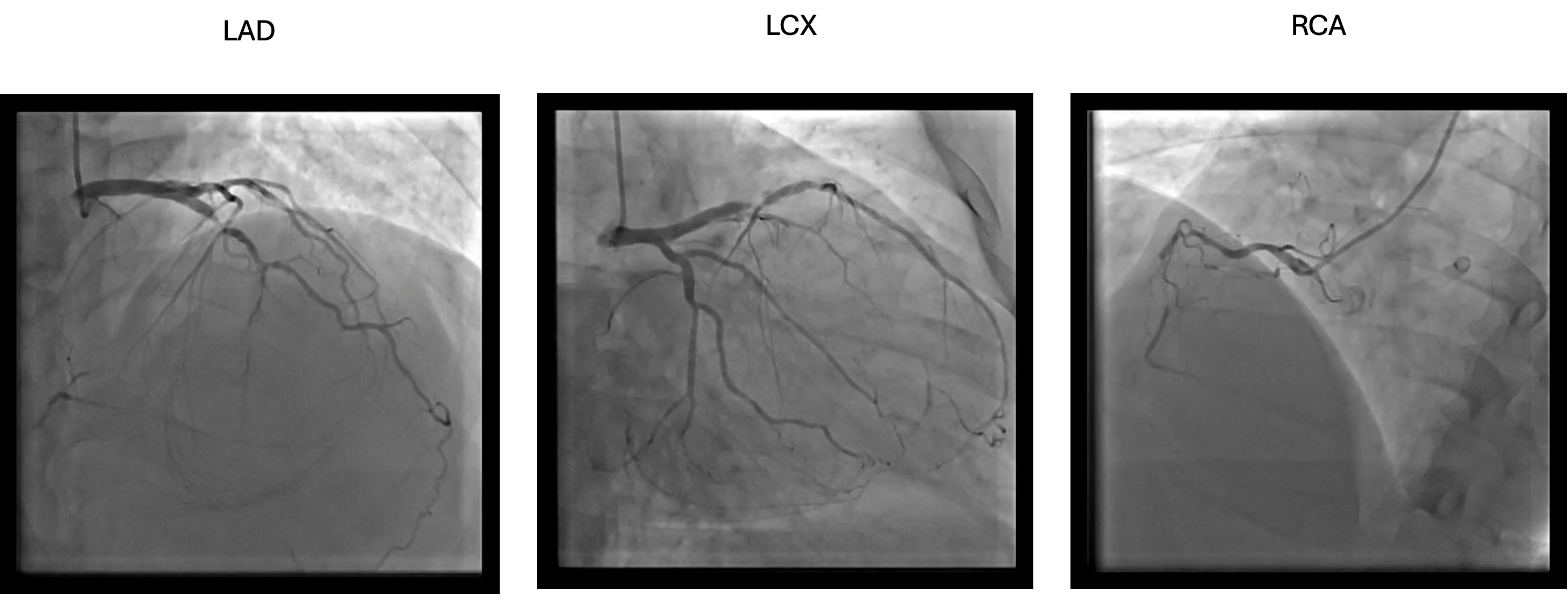
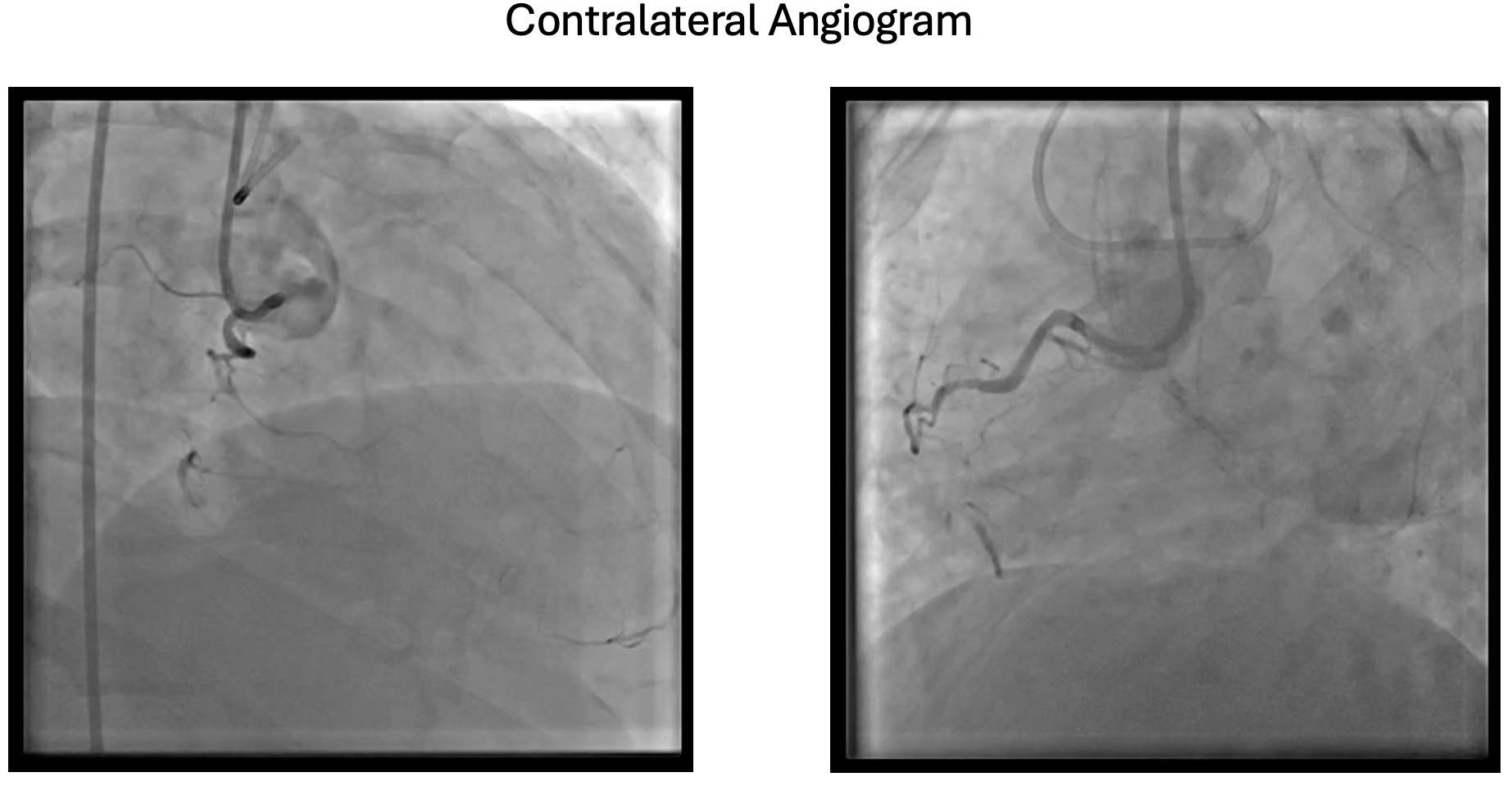
55 year old man with underlying severe plaque psoriasis on s/c ustekinumab had an anterior myocardial infarction in 2012 while travelling. He was not offered thromblysis and had only underwent angiogram 2 weeks later after returning and LAD was stented. In 2023, he had NSTEMI and during that time, his ejection fraction had worsen to 30% and cardiac MRI showed non viable LAD. Repeated angiogram showed ISR 99% of LAD, recessive LCX and CTO dominant RCA.
Relevant Test Results Prior to Catheterization
Cardiac MRI : Ischemic dilated cardiomyopathy with moderate LV systolic dysfunction ( LVEF 32% ) and normal RV systolic dysfunction ( RVEF 58% ). Minimal viability seen within mid to apical anterior, mid to apical anterior-septum and all apical segments ( Non viable mid LAD territory ) . All other segments are viable
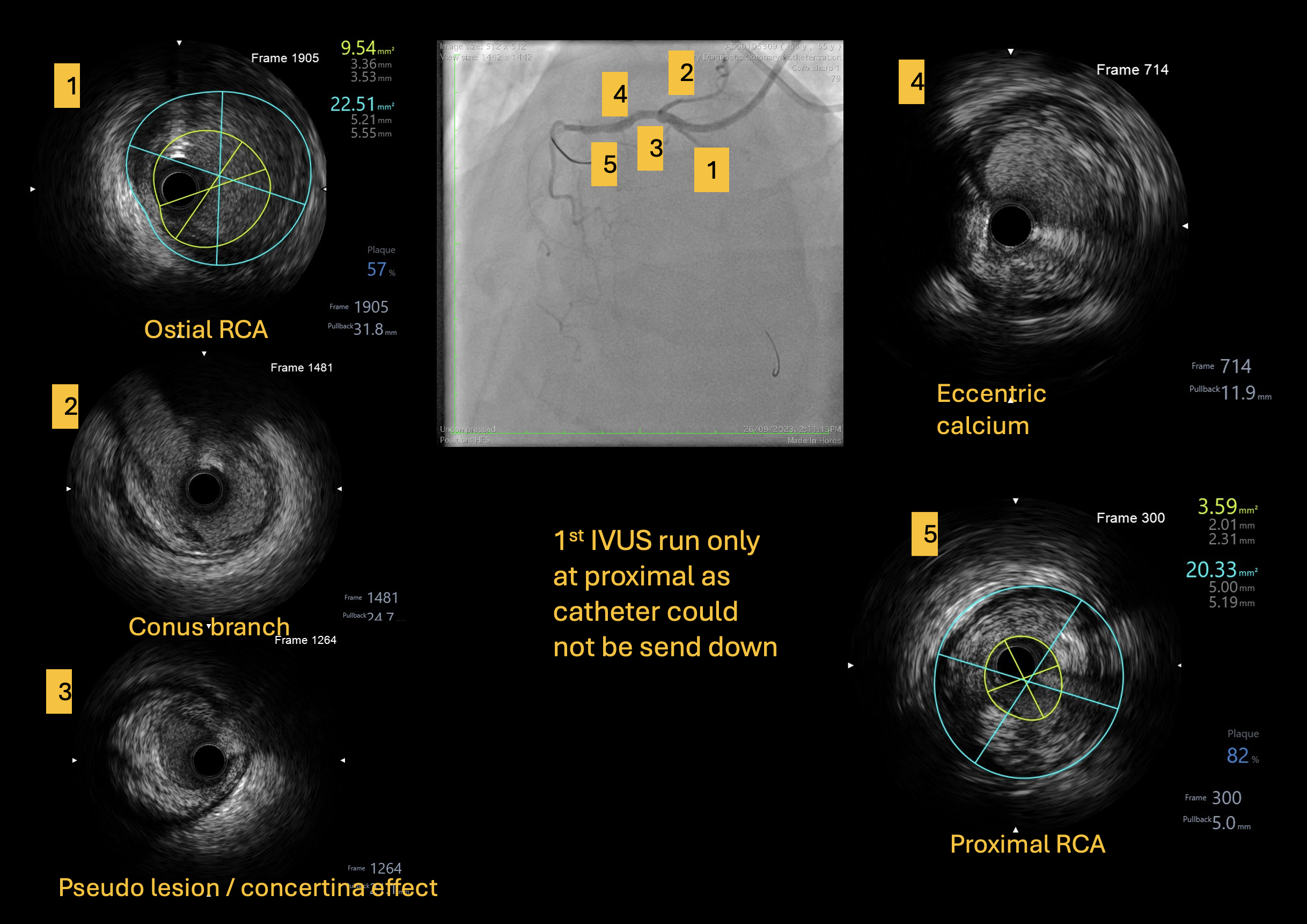
Relevant Catheterization Findings
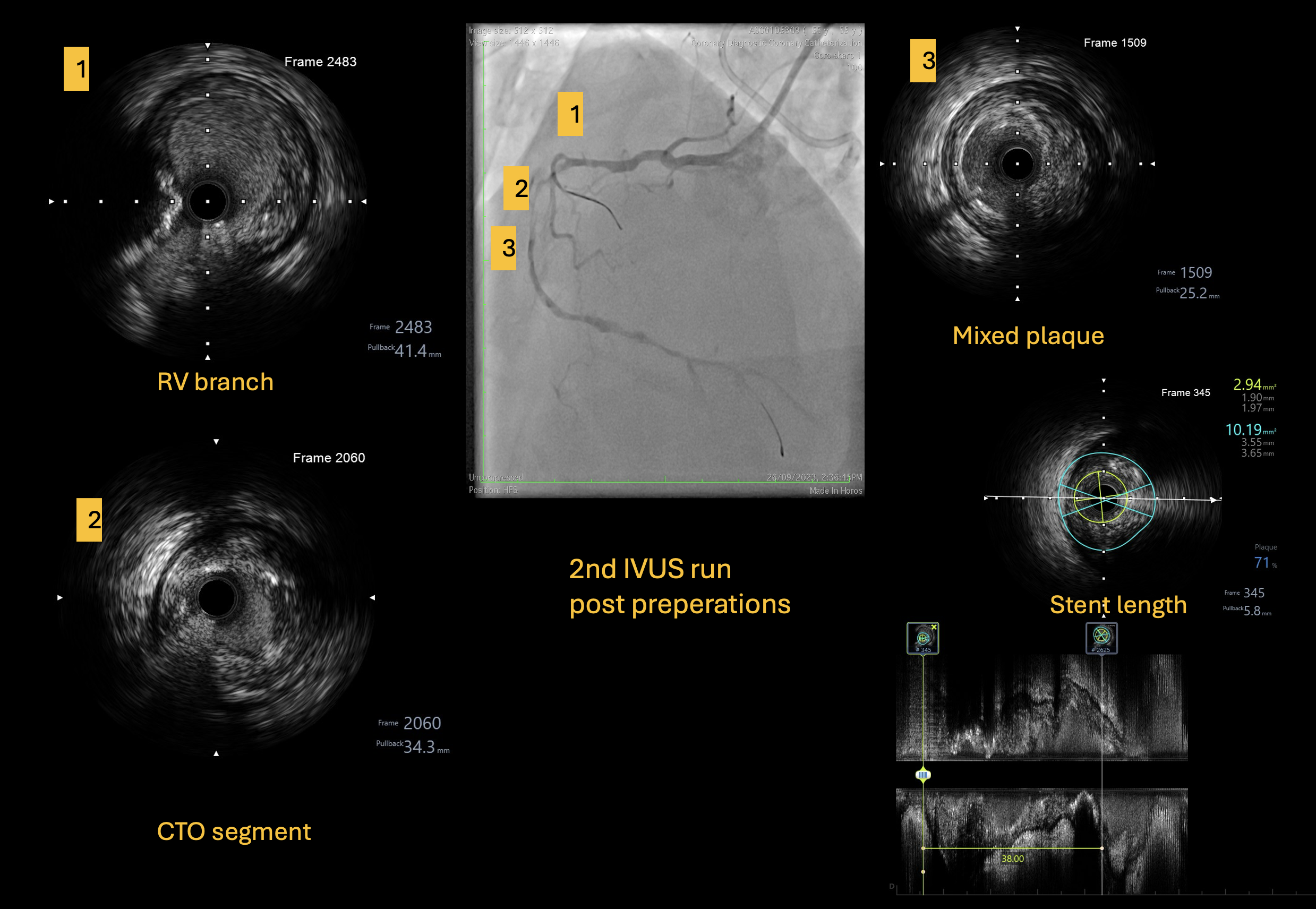
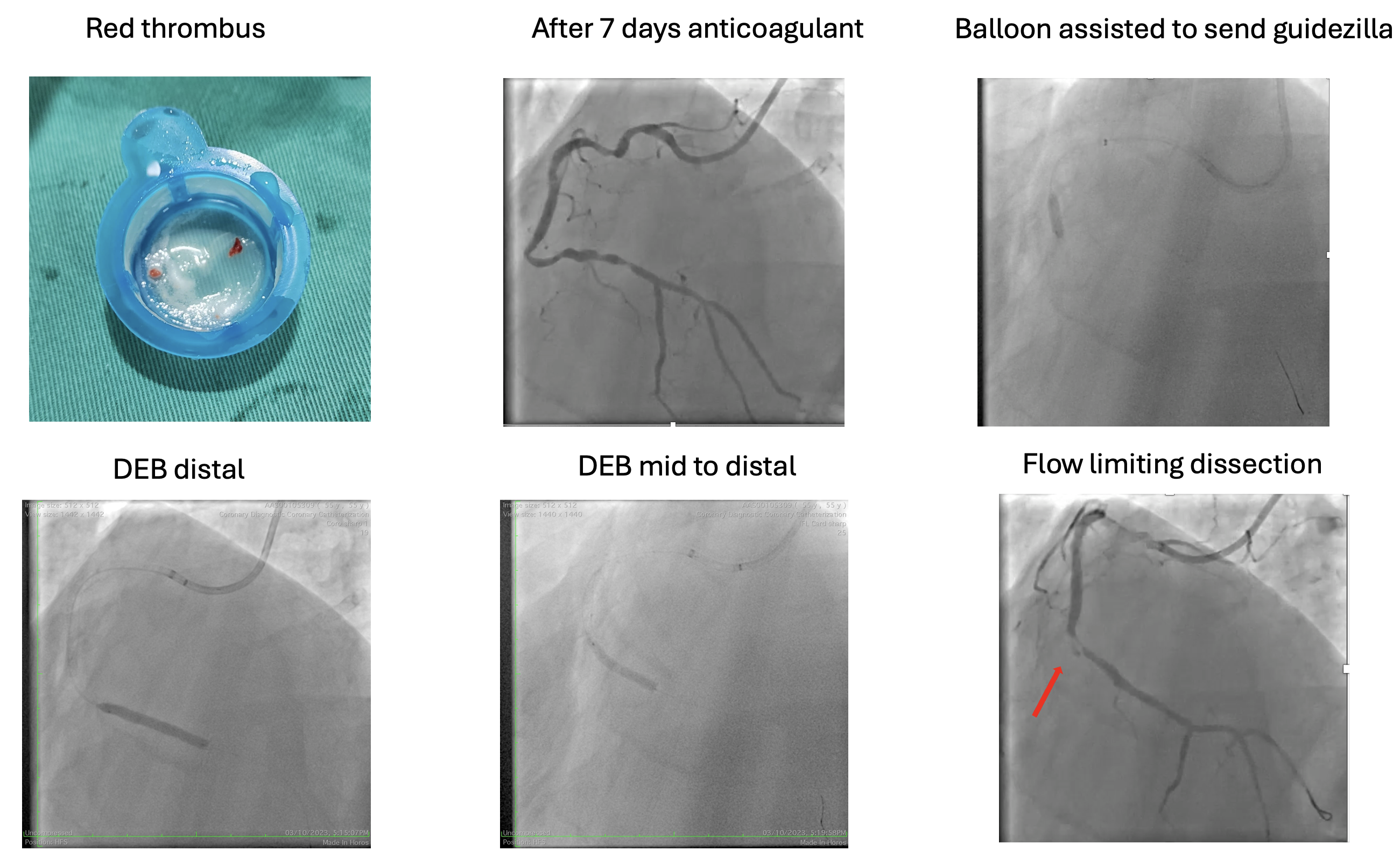
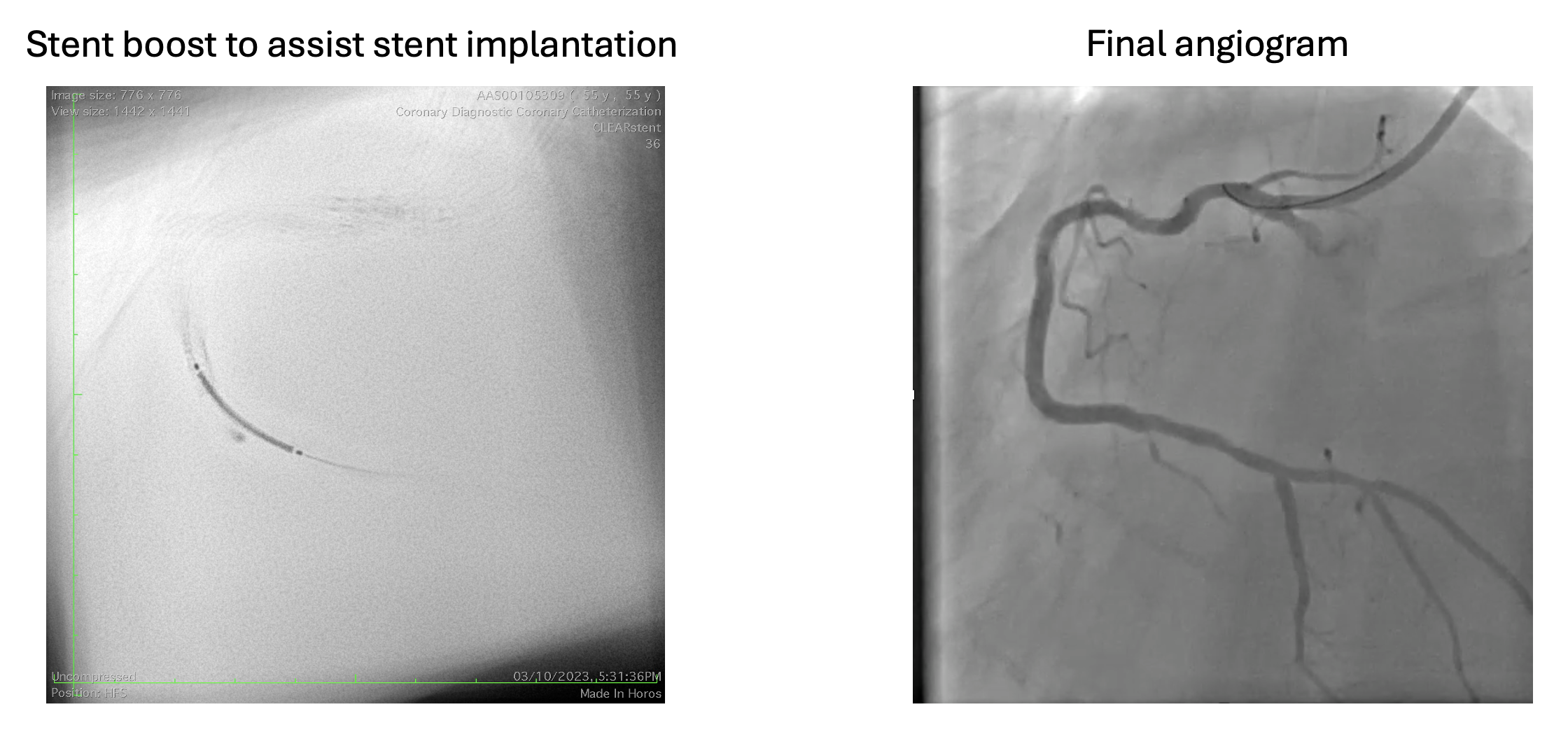
Interventional Management
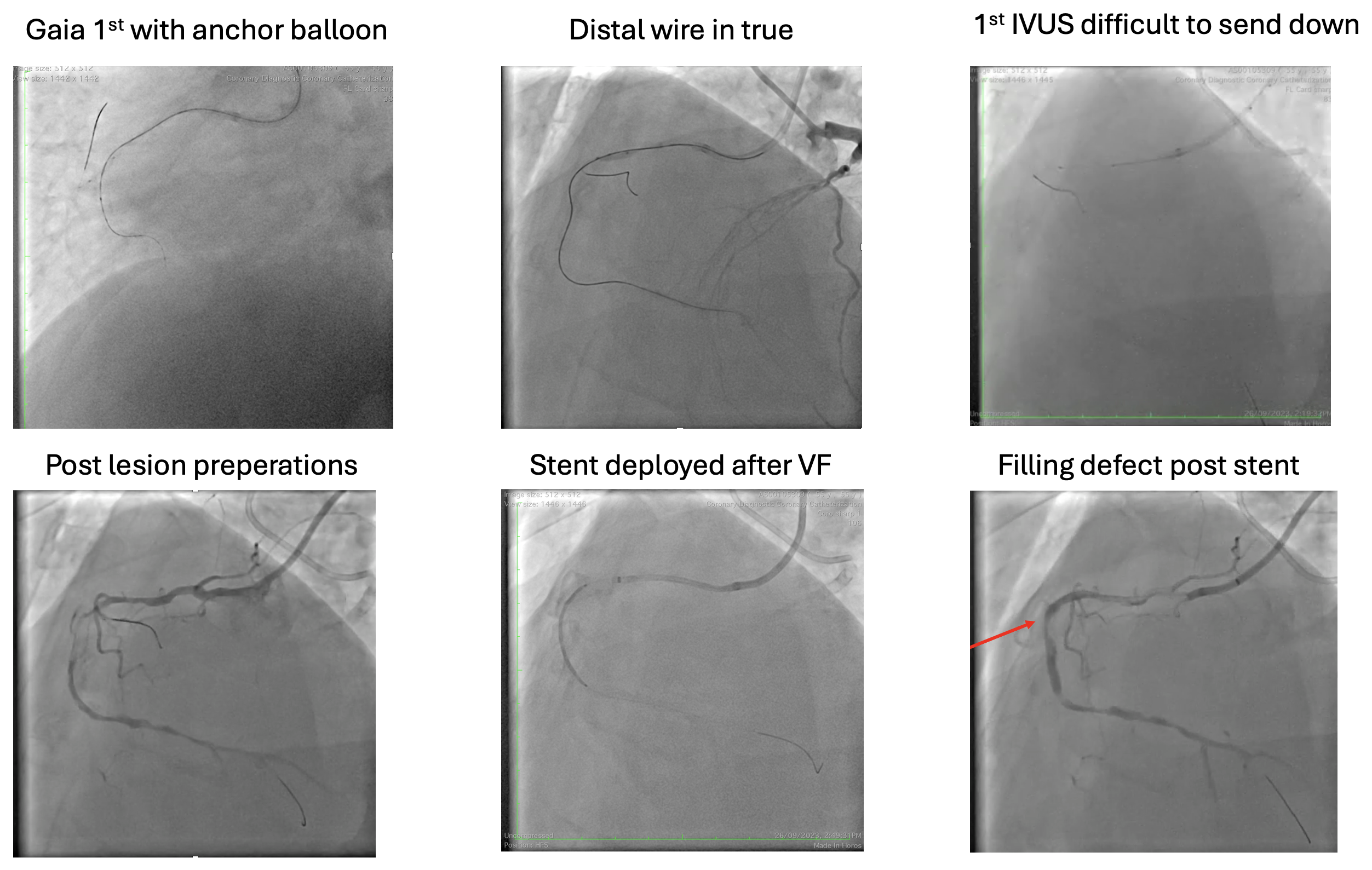
Procedural Step
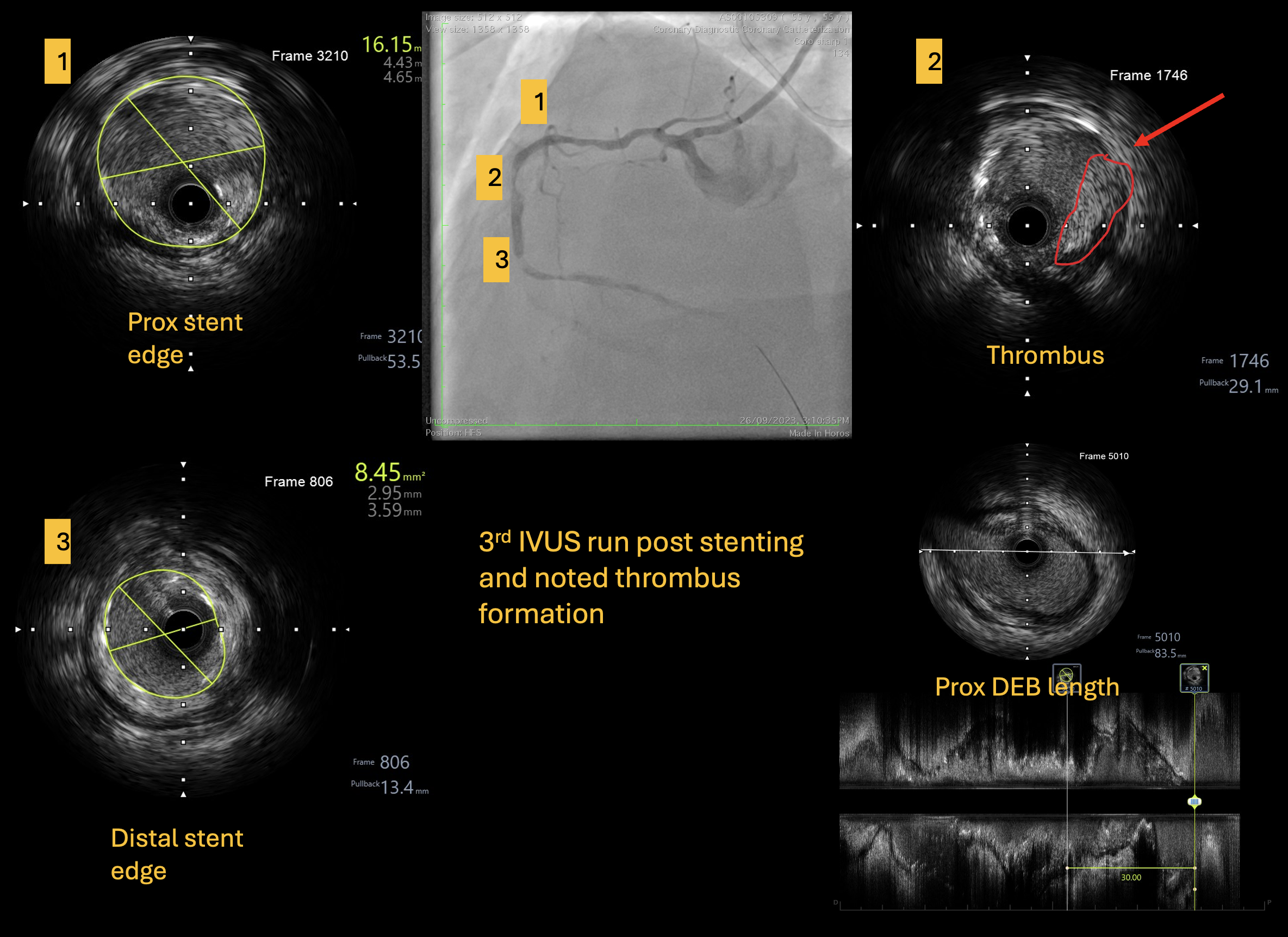
Case Summary
Patient well and his EF had improved from 30% to 40% and now symptoms free. During the procedure, we wondered why patient had thrombosis despite ACTs were adequate. We found out that s/c ustekinumib, the biologics used for his psoriasis had been reported to have increased incidence of thrombosis. Other learning points in this case are tortuous vessel is the bane of intervention, even more so in CTOi. Next in tortuous vessels, wires, IVUS and Guidezilla can cause pseudo lesion, also known as concertina effect. DCB can be a good option in tortuous vessels if proper preparations is done and always be prepared with managing flow limiting dissection.