
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-118
Float and Flare: Critical Ostial Left Main Stenting
By Shen Yew Yee, Ramachandran Sathappan, Gurpreet Pal Singh Jugindar Singh, Chun Liang Lim, Jian-Gang Ang, Zarrin Kang, Tai Meng Chen, Yew Fung Kwan, Hazleena Mohamed Hasnan, Nor Hanim Mohd Amin
Presenter
Shen Yew Yee
Authors
Shen Yew Yee1, Ramachandran Sathappan1, Gurpreet Pal Singh Jugindar Singh1, Chun Liang Lim1, Jian-Gang Ang1, Zarrin Kang1, Tai Meng Chen1, Yew Fung Kwan1, Hazleena Mohamed Hasnan1, Nor Hanim Mohd Amin1
Affiliation
Hospital Raja Permaisuri Bainun, Malaysia1,
View Study Report
TCTAP C-118
Coronary - Complex PCI - Left Main
Float and Flare: Critical Ostial Left Main Stenting
Shen Yew Yee1, Ramachandran Sathappan1, Gurpreet Pal Singh Jugindar Singh1, Chun Liang Lim1, Jian-Gang Ang1, Zarrin Kang1, Tai Meng Chen1, Yew Fung Kwan1, Hazleena Mohamed Hasnan1, Nor Hanim Mohd Amin1
Hospital Raja Permaisuri Bainun, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Madam TSL, a 51-year-old woman with underlying hypertension and history of recurrent chest pain. She presented with non-ST elevation acute coronary syndrome in April 2024. Physical examinations were unremarkable.
Relevant Test Results Prior to Catheterization
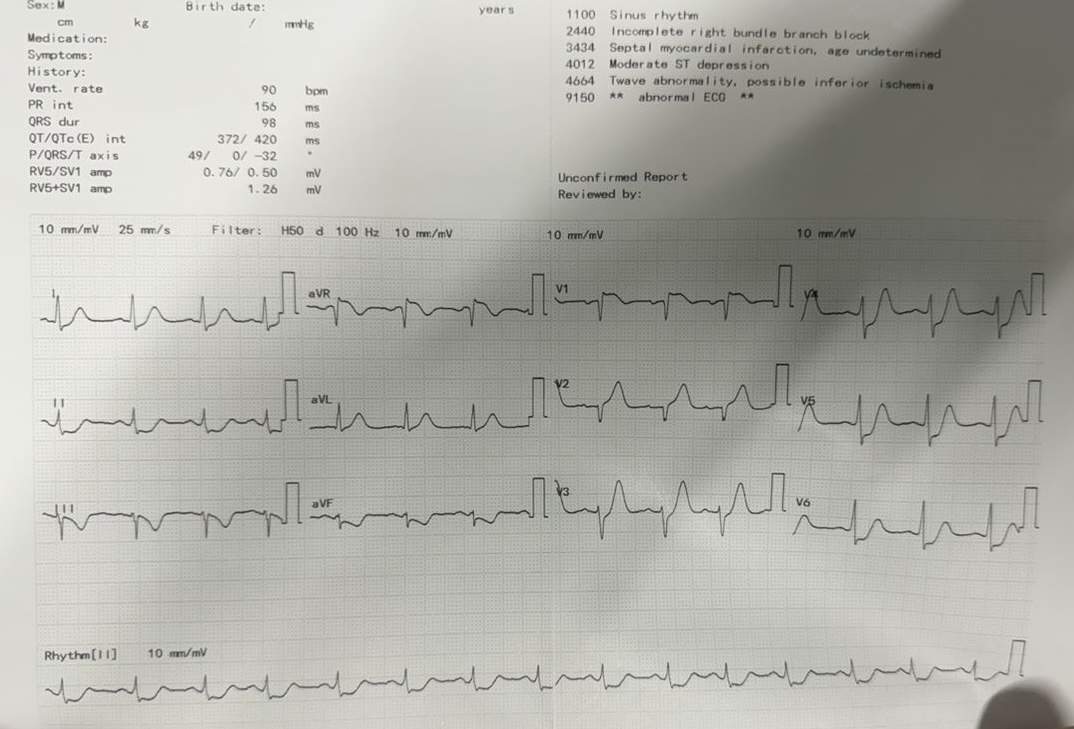
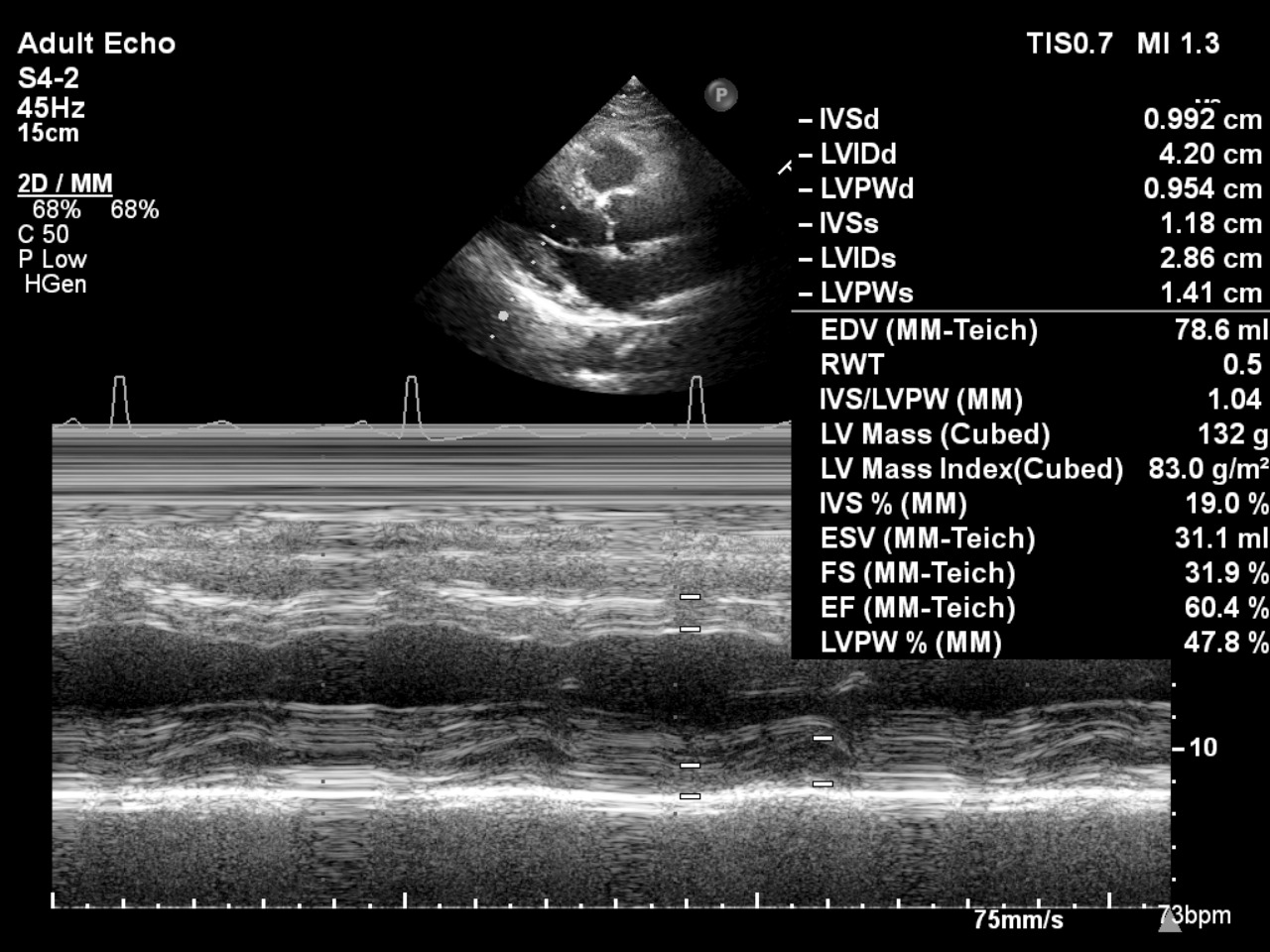
Electrocardiogram: ST elevation in aVR and V1 with widespread ST depressionEchocardiography: EF 60.4% with anteroseptal hypokinesia. No significant valvular abnormalities.
Hemoglobin: 12g/dLPlatelet: 263x109/LUrea: 3.7mmol/LCreat: 61umol/LeGFR: >90ml/min/1.73m2Troponin I raised
Hemoglobin: 12g/dLPlatelet: 263x109/LUrea: 3.7mmol/LCreat: 61umol/LeGFR: >90ml/min/1.73m2Troponin I raised
Relevant Catheterization Findings
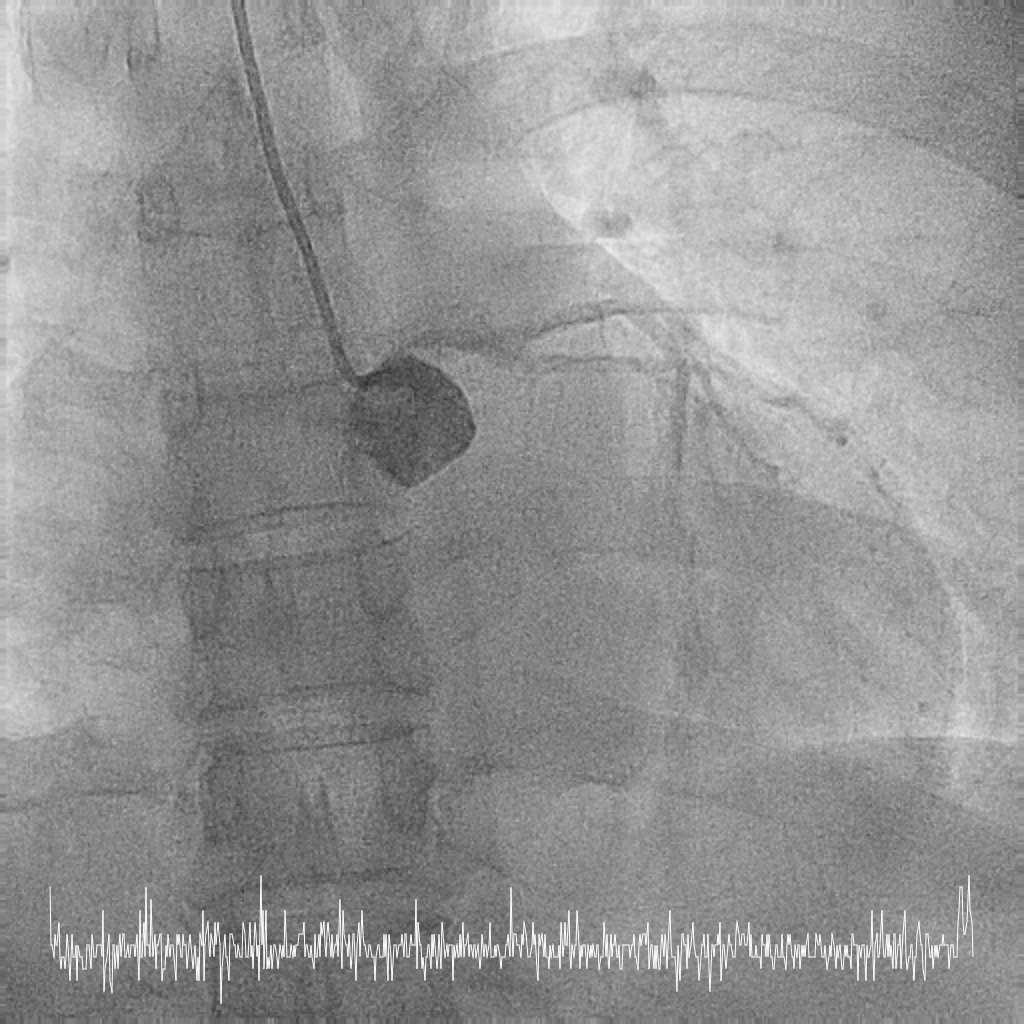
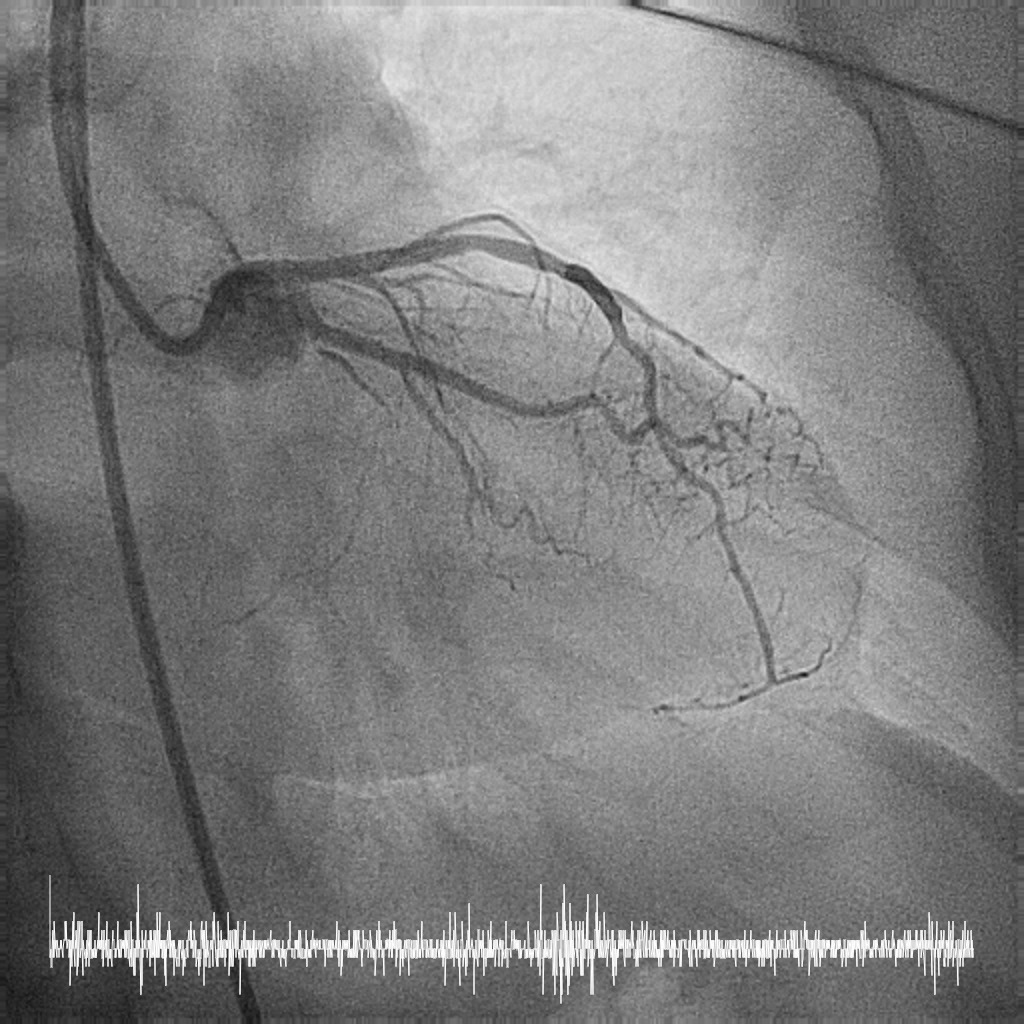
Coronary angiography performed via right radial approach with a 5F Optitorque diagnostic catheter.
LMS: Ostia LMS 99% stenosis with pressure dampingLAD: Proximal LAD 30-40% stenosisLCx: NormalRCA: Dominant. Normal.
Patient developed short run VT during engagement to left main.
She was referred for coronary artery bypass graft however the patient strongly refused, hence the decision for CHIP-PCI to an unprotected, severely stenotic left main artery.


LMS: Ostia LMS 99% stenosis with pressure dampingLAD: Proximal LAD 30-40% stenosisLCx: NormalRCA: Dominant. Normal.
Patient developed short run VT during engagement to left main.
She was referred for coronary artery bypass graft however the patient strongly refused, hence the decision for CHIP-PCI to an unprotected, severely stenotic left main artery.
Interventional Management
Procedural Step
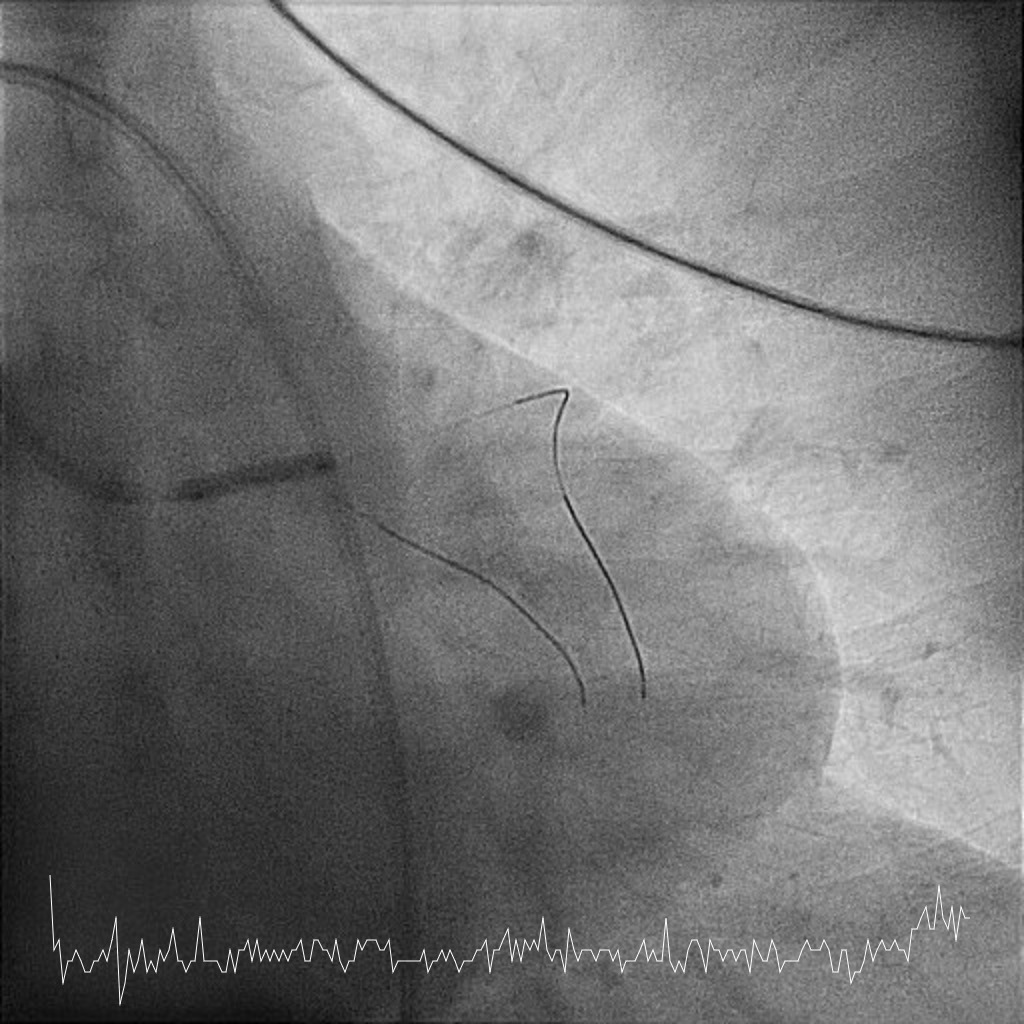
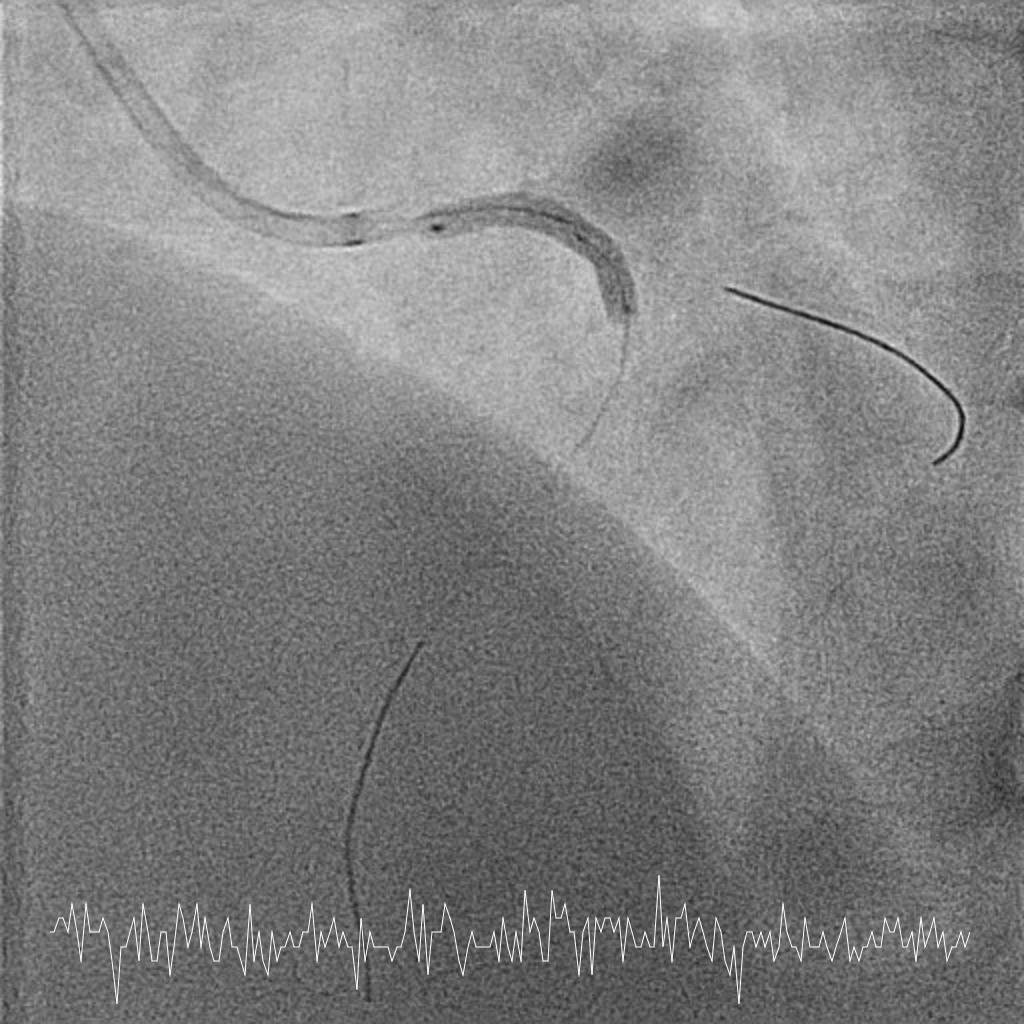
Femoral approach was chosen with a 7F sheath. A 7F JL4 guiding catheter was used for better support. JL4 was not coaxially engaged but positioned close to the ostial LM. Sion Blue ES was wired into LAD from the aortic cusp. A BMW wire was wired into LCx to provide additional support and as a safety wire in case of plaque shift into ostial LCx. Ostial LM was predilated with 3.0/10mm NC balloon at 12ATM which was delivered via Sion Blue ES with the guide and wire floating in the aorta. IVUS after predilatation revealed an ostial LM MLA 5.28mm2 with vessel size 4.0mm. Proximal LAD measured 3.0mm in size and exhibited fibrotic plaque with 70% plaque burden. Both ostial LM and proximal LAD were predilated with 3.0/15mm NC balloon delivered using the floating guide and Sion Blue ES. A 3.0/33mm DES was delivered and deployed with similar technique into proximal LAD using multiple projections for precise positioning to ensure proximal stent edge protrusion of 1-2mm into the aorta. POT of LM and ostial flare were performed using 3.75/15mm NC balloon. Proximal LAD was postdilated with 3.0/15mm NC balloon. IVUS confirmed a well-opposed stent without stent edge dissection. The final ostial LM MSA was 9.7mm2, with stent protrusion (1.7mm) into the aorta (less than one quadrant). The entire ostial LM was covered with stent struts.
Case Summary
A less aggressive JL4 facilitated close positioning to the ostial LM without coaxial engagement, allowing easy disengagement during equipment withdrawal. Extra support wire like Sion Blue ES is crucial for device delivery when guide support is limited. Precise stent positioning using multiple projections is critical for optimal ostial LM stenting. The ostial flare technique simplifies future engagement for potential ostial interventions. While techniques like Sepal and Szabo technique have been described, current evidence suggests limited accuracy and risk of excessive stent protrusion into the aorta.