
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-070
Rear-Ended!: An Unexpected Development During Percutaneous Coronary Intervention for Chronic Total Occlusion
By Ying-Chien Wang
Presenter
Ying-Chien Wang
Authors
Ying-Chien Wang1
Affiliation
Changhua Christian Hospital, Taiwan1,
View Study Report
TCTAP C-070
Coronary - Complex PCI - CTO
Rear-Ended!: An Unexpected Development During Percutaneous Coronary Intervention for Chronic Total Occlusion
Ying-Chien Wang1
Changhua Christian Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 57-year-old man with underlying hypertension and hyperuricemia presented to our emergency department with intermittent chest pain for 3 days. Cardiac enzymes were elevated (hs-Troponin I: 2749.1 ng/L, creatine kinase: 207 U/L, CK-MB: 13.0 ng/mL) and he was diagnosed with non-ST elevation myocardial infarction.
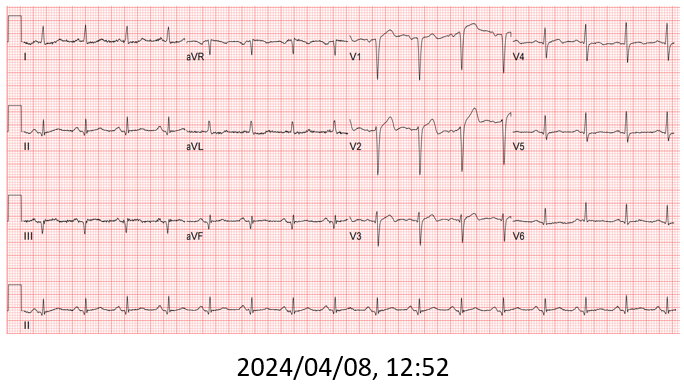
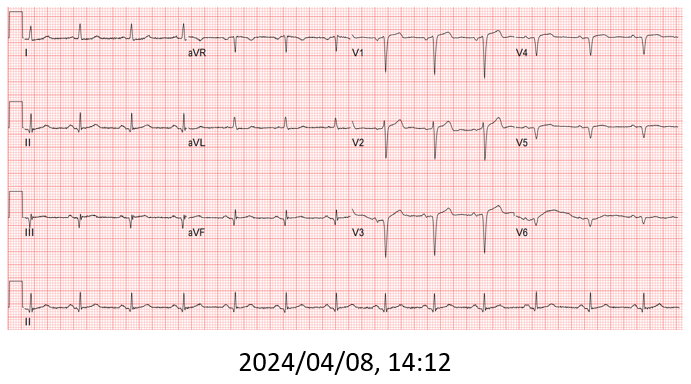

Relevant Test Results Prior to Catheterization
Coronary angiogram found 3-vessel disease with middle left anterior descending artery (LAD) total occlusion, and middle left circumflex (LCx) plus middle right coronary artery (RCA) chronic total occlusion (CTO).
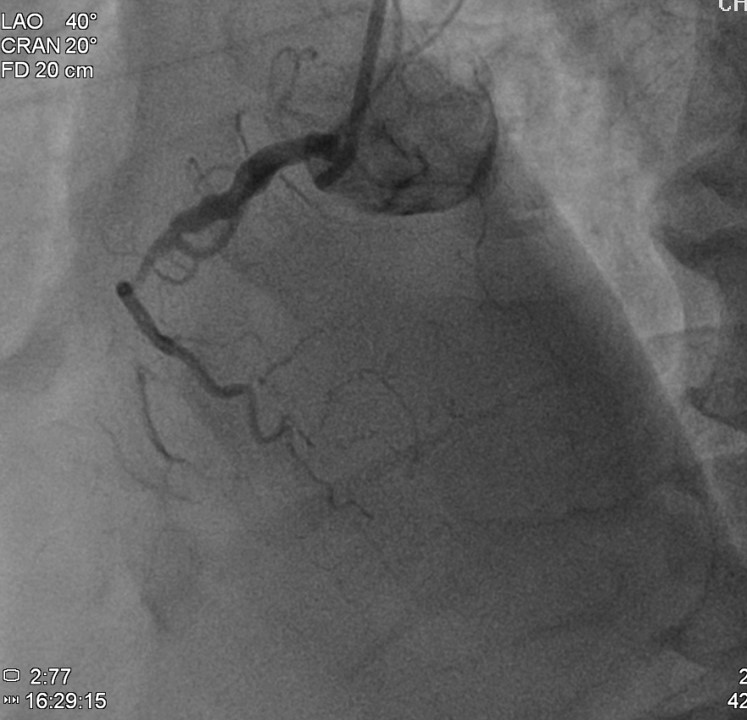

Relevant Catheterization Findings
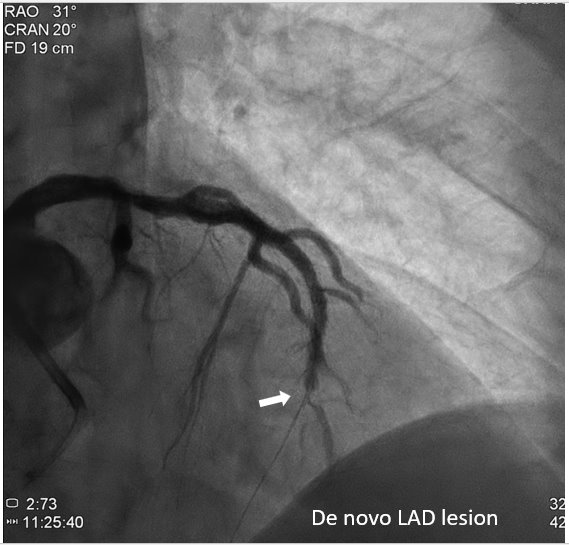
The patient received primary percutaneous coronary intervention (PCI) with balloon angioplasty (POBA) and a drug-eluted stent (DES) for middle LAD. Three days later he underwent staged PCI for RCA. After wire externalization via rendezvous technique, the patient developed acute angina, diaphoresis, and hypotension. Angiogram found a de-novo LAD lesion just distal to the stent.
Interventional Management
Procedural Step
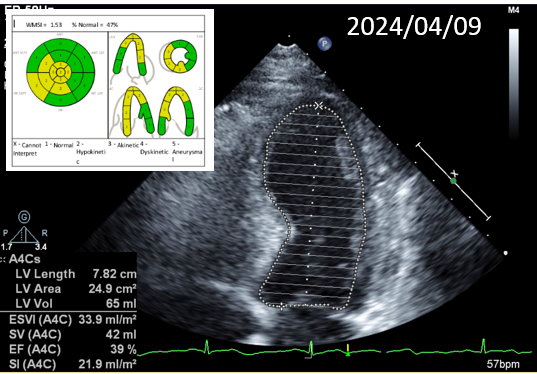
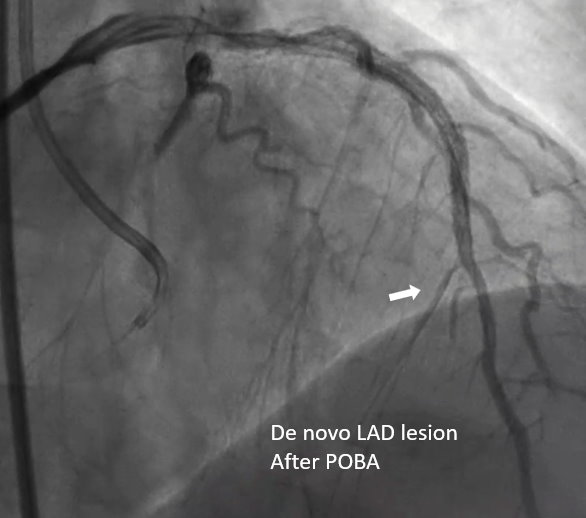
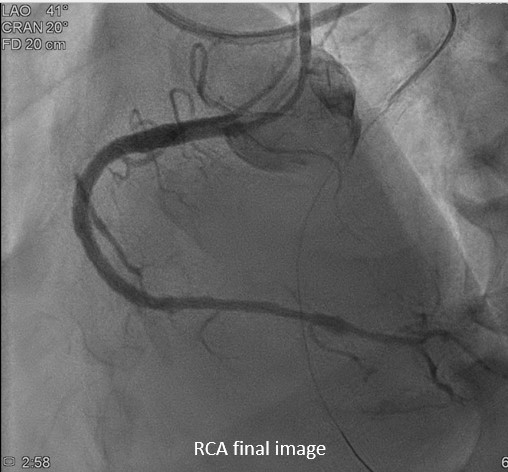
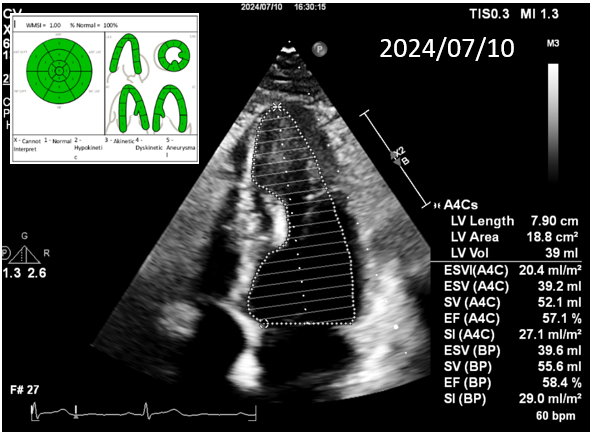
During the staged PCI, antegrade approach with escalating guidewires ended up in subintimal space; retrograde approach from the first LAD-septal branch failed because there was difficulty crossing the existing mid-LAD stent. Further attempts from the third septal branch successfully reached the distal cap of the CTO via proximal descending artery, finally entering the antegrade guide extension catheter by rendezvous technique. After wire externalization and POBA for RCA, the patient became agitated from acute angina, diaphoresis and hypotension. Angiogram of LAD found an acute de novo LAD lesion adjacent to the distal stent edge, leaving only TIMI-1 flow. We stopped the RCA procedure and wired LAD, performed POBA at the de novo LAD lesion and restored coronary blood flow. Then we continued PCI of RCA with POBA followed by the deployment of two DES. Final angiogram showed adequate stent expansion and TIMI-3 flow in RCA. The patient was discharged with no further complications. Follow-up echocardiogram three months later showed improved wall motion and ejection fraction, indicating good myocardial recovery.
Case Summary
While treating CTO lesions, the operator may become tunnel-visioned and focus only on the target. In our case, however, the retrograde side (LAD) developed a de novo lesion, possibly resulting from wire manipulation during the initial failed retrograde approach and at externalization. The "rear-end impact" led directly to patient instability and it is worth keeping in mind that this can be a cause of periprocedural complication.