
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-083
Overcoming the Challenges of Calcification at the Angulation Within RCA CTO: Successful Revascularization With Tip-in Wire Rendezvous Technique
By Wang Yeh Ling, Yi-Chih Wang
Presenter
Wang Yeh Ling
Authors
Wang Yeh Ling1, Yi-Chih Wang1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-083
Coronary - Complex PCI - CTO
Overcoming the Challenges of Calcification at the Angulation Within RCA CTO: Successful Revascularization With Tip-in Wire Rendezvous Technique
Wang Yeh Ling1, Yi-Chih Wang1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This is a 51-year-old man with a past medical history of hypertension, diabetes mellitus, dyslipidemia, and chronic coronary syndrome. Coronary angiography was performed at a local hospital, revealing left main (LM) disease and chronic total occlusion (CTO) at the distal right coronary artery (RCA). A drug-eluting stent (DES) was successfully deployed in the LM-LAD, but an attempt to treat the RCA CTO failed. The patient subsequently sought further medical assistance at our hospital.
Relevant Test Results Prior to Catheterization
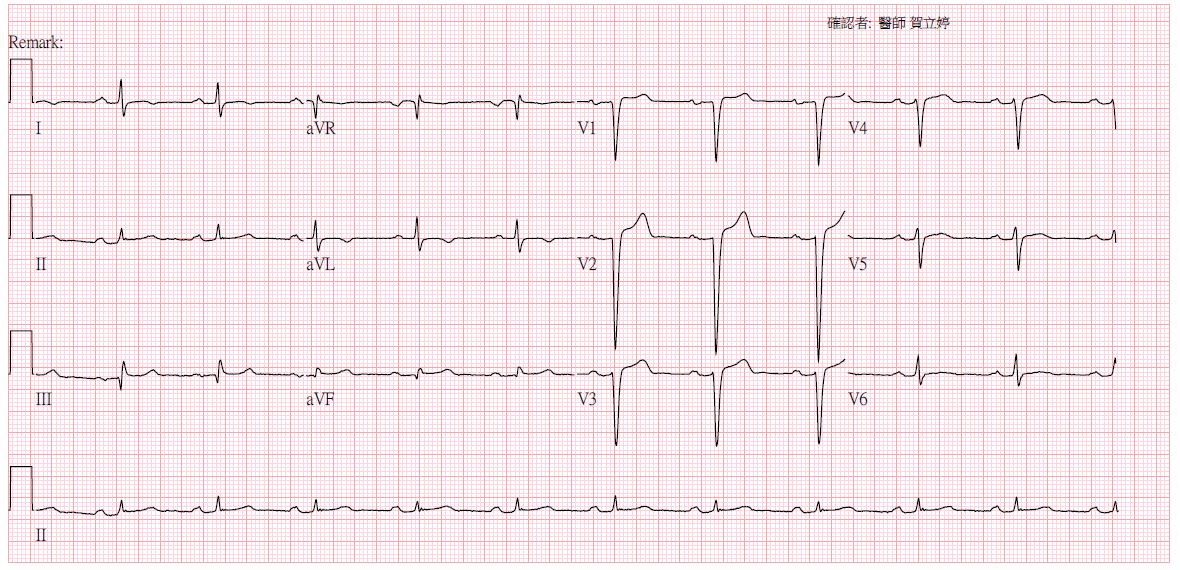
Electrocardiography before the procedure showed sinus rhythm with poor R-wave progression.
Relevant Catheterization Findings
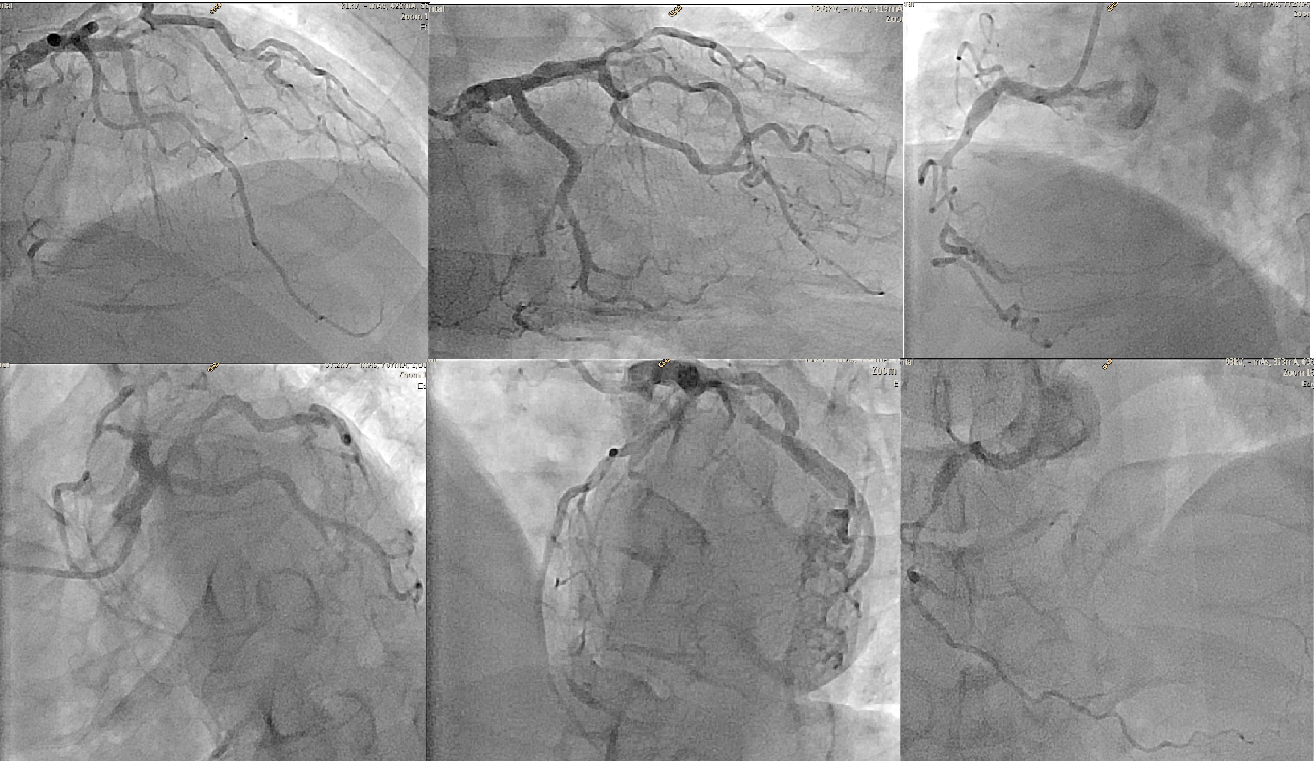
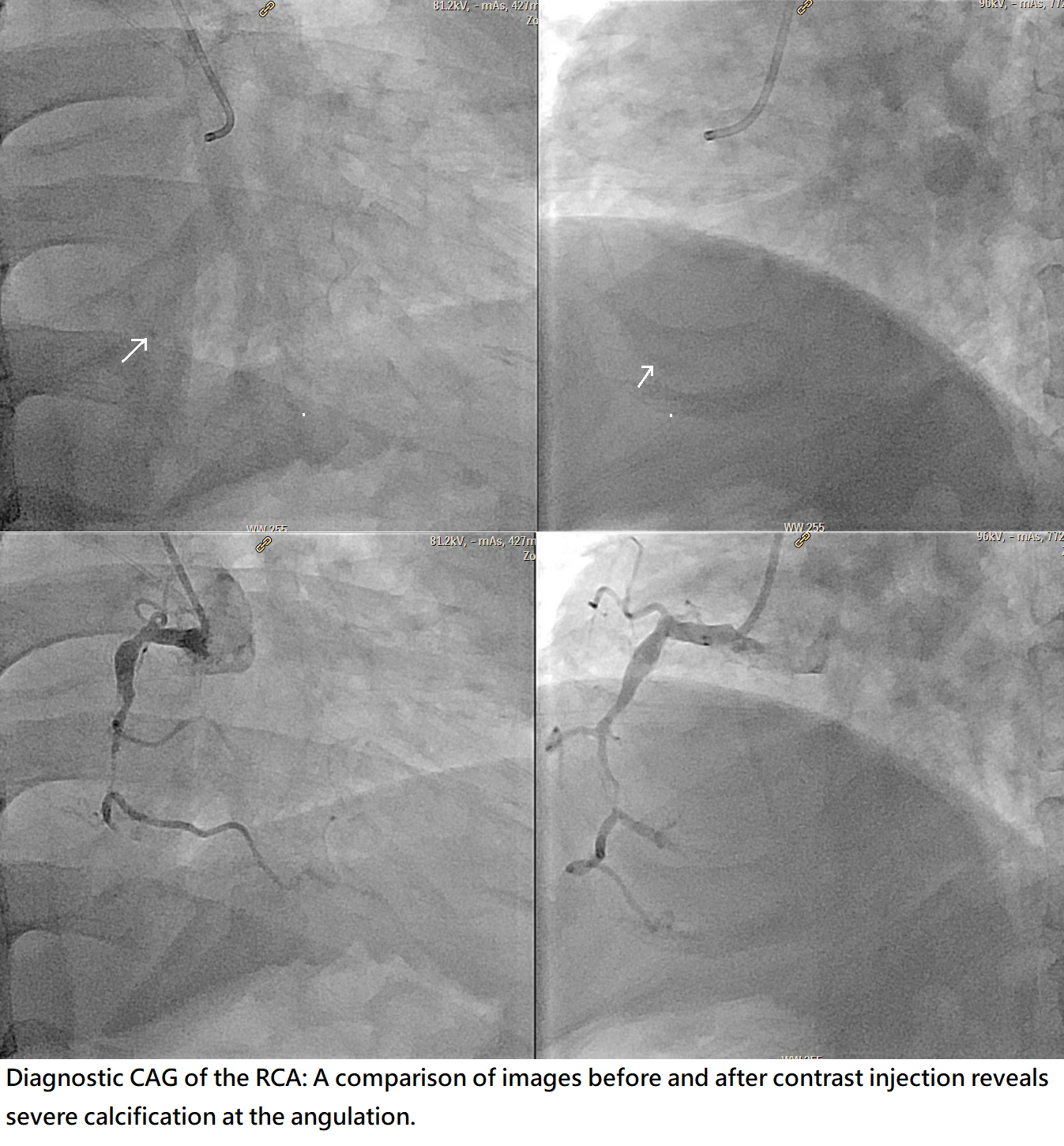
Coronary angiography revealed no in-stent restenosis in the LM-LAD stent and no significant stenosis in the LAD or LCx. The septal branch provided collateral flow to the posterior descending artery (PDA), while the LCx supplied collateral flow via small atrioventricular (AV) groove collaterals. Multiple stenotic lesions were identified in the RCA, including a discrete lesion in the proximal RCA, a long lesion with up to 90% stenosis in the mid RCA, and a calcified CTO lesion in the distal RCA.
Interventional Management
Procedural Step
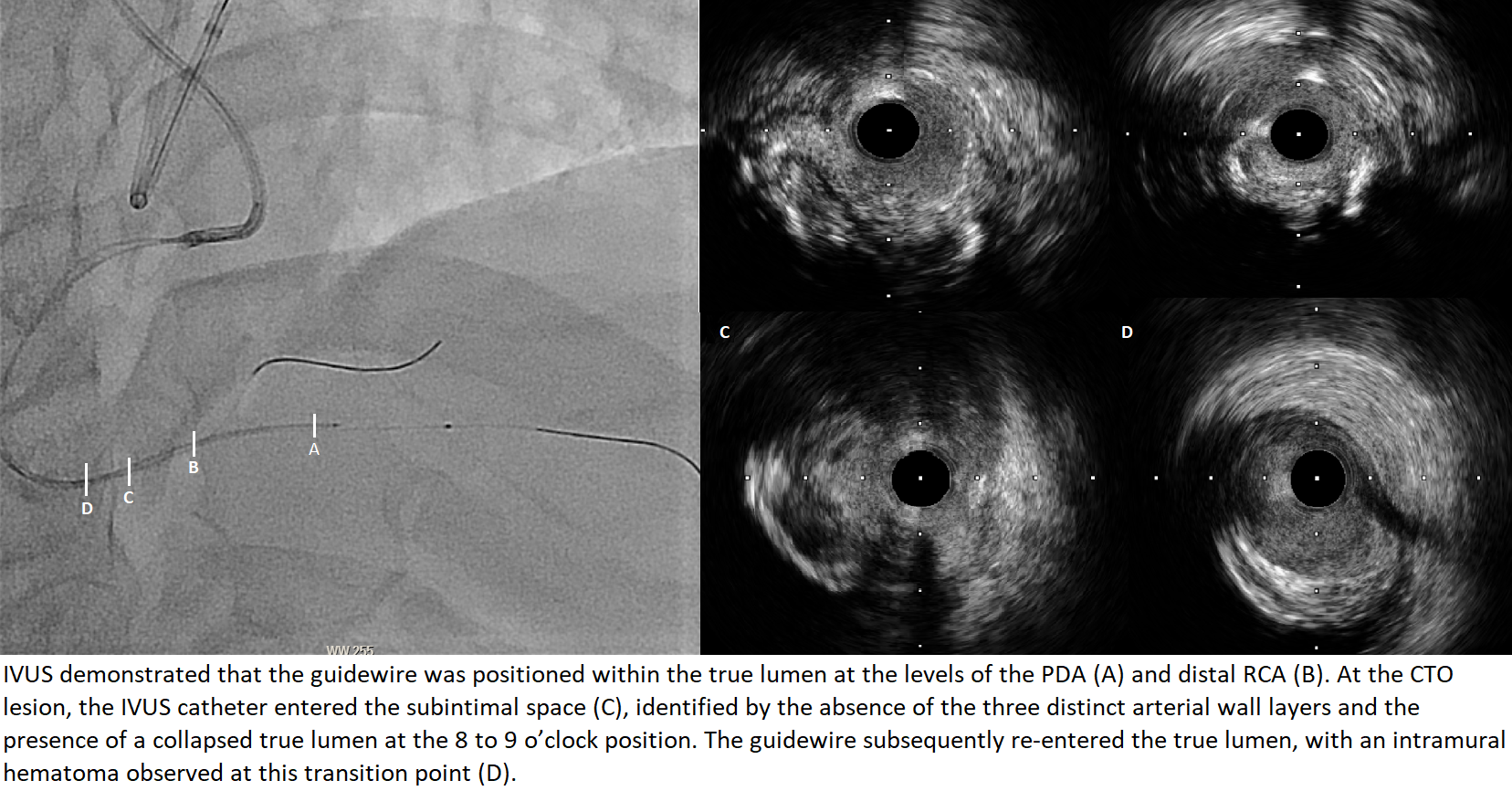
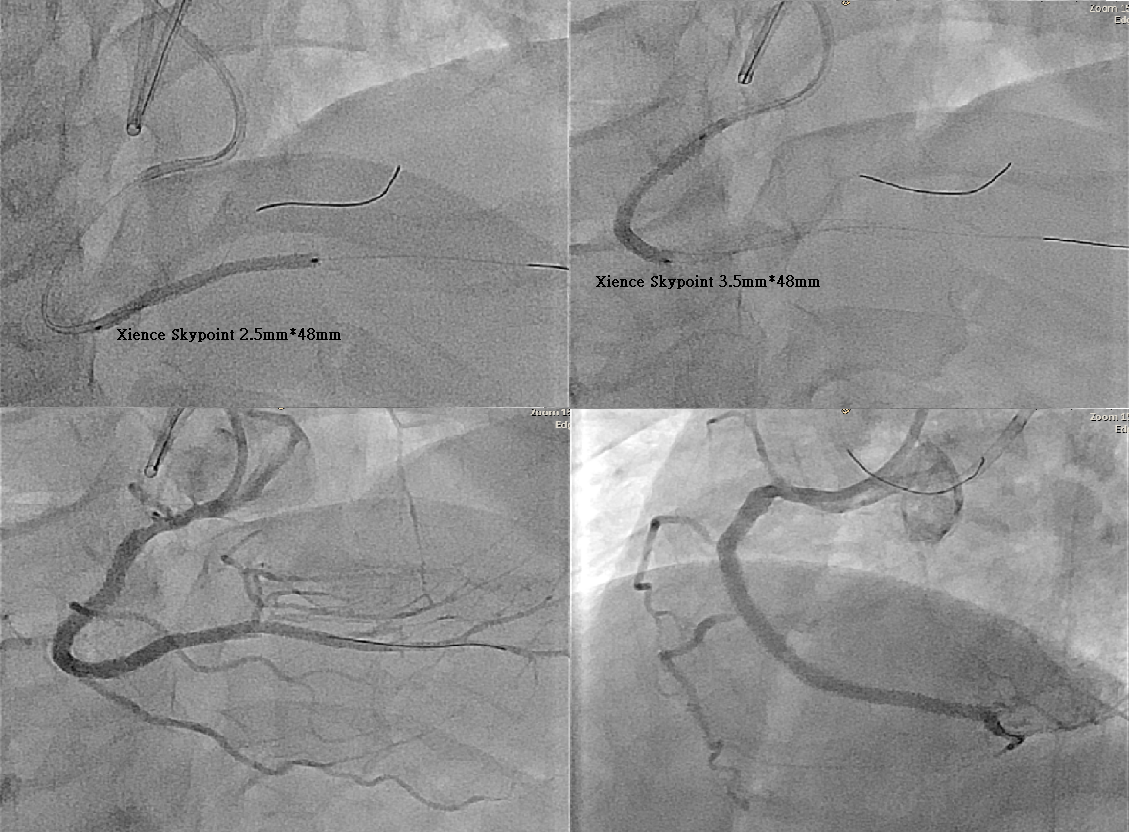
1. Dual injection was performed using a transradial approach: LRA with an AL 1/6 Fr GC and RRA with an EBU 3.5/7 GC.2. Fielder XT-R, Fielder FC, and GAIA Second were deviated into subintima by the calcification at the angulation and failed to cross the CTO antegradely with a Corsair MC.3. SUOH 03 successfully crossed the septal collaterals using a Caravel MC and reached the distal RCA.4. Sion Black and Fielder XT-A were also deviated into subintima by the calcification at the angulation and failed to cross the CTO retrogradely.5. Attempts to use the kissing wire technique with Conquest Pro, Conquest Pro 8-20, and GAIA Third were unsuccessful due to the hindrance of calcification.6. Using the reverse CART technique, the CTO lesion was crossed retrogradely, and the Fielder FC was advanced into the antegrade GC.7. When the retrograde Caravel could not advance into the antegrade GC due to the calcification, the tip-in wire rendezvous method was used as a bailout: the Fielder FC wire was advanced into the antegrade Corsair MC in the antegrade GC, and the antegrade MC successfully crossed the CTO lesion via the retrograde guidewire.8. Sion Blue was then used as the antegrade workhorse wire, placed to PDA.9. IVUS revealed a diffuse lesion in the RCA with the guidewire positioned within the true lumen , except for a short subintimal segment just at the calcification within the CTO angulation.10. Two long DESs were deployed at the RCA-PDA and p-dRCA. Final angiography confirme TIMI-3 flow.
Case Summary
This case highlights several considerations for CTO-PCI management. First, acute angulation within the CTO usually leads to wiring deviation, either by antegrade or retrograde techniques. Second, severe calcification at the angulation would much increase the wiring difficulty. As the presenting case, while the retrograde wire escalation/de-escalation and kissing wire techniques were initially attempted to minimize subintimal tracking, the reverse CART technique was the key procedure to overcome such kind of challenge. Third, when the retrograde microcatheter failed to advance into the antegrade guide catheter, the tip-in wire rendezvous method was proved to be an effective bailout.