
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-085
An Extreme Elderly Patient With Double CTO
By Ming Leo Lau, Ho Fai Daniel Fong
Presenter
Ming Leo Lau
Authors
Ming Leo Lau1, Ho Fai Daniel Fong1
Affiliation
Yan Chai Hospital, Hong Kong, China1,
View Study Report
TCTAP C-085
Coronary - Complex PCI - CTO
An Extreme Elderly Patient With Double CTO
Ming Leo Lau1, Ho Fai Daniel Fong1
Yan Chai Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This is a 80 years' old gentleman who was a non-smoker and ex-drinker. He had medical history of hypertension, gout and gallbladder stones. He had suffered from on and off chest pain since 2 weeks ago and had increased chest pain on the day of admission. Physical exam showed stable vital signs. Chest examination found no wheeze or crepitations. Cardiac exam found no heart murmurs.
Relevant Test Results Prior to Catheterization
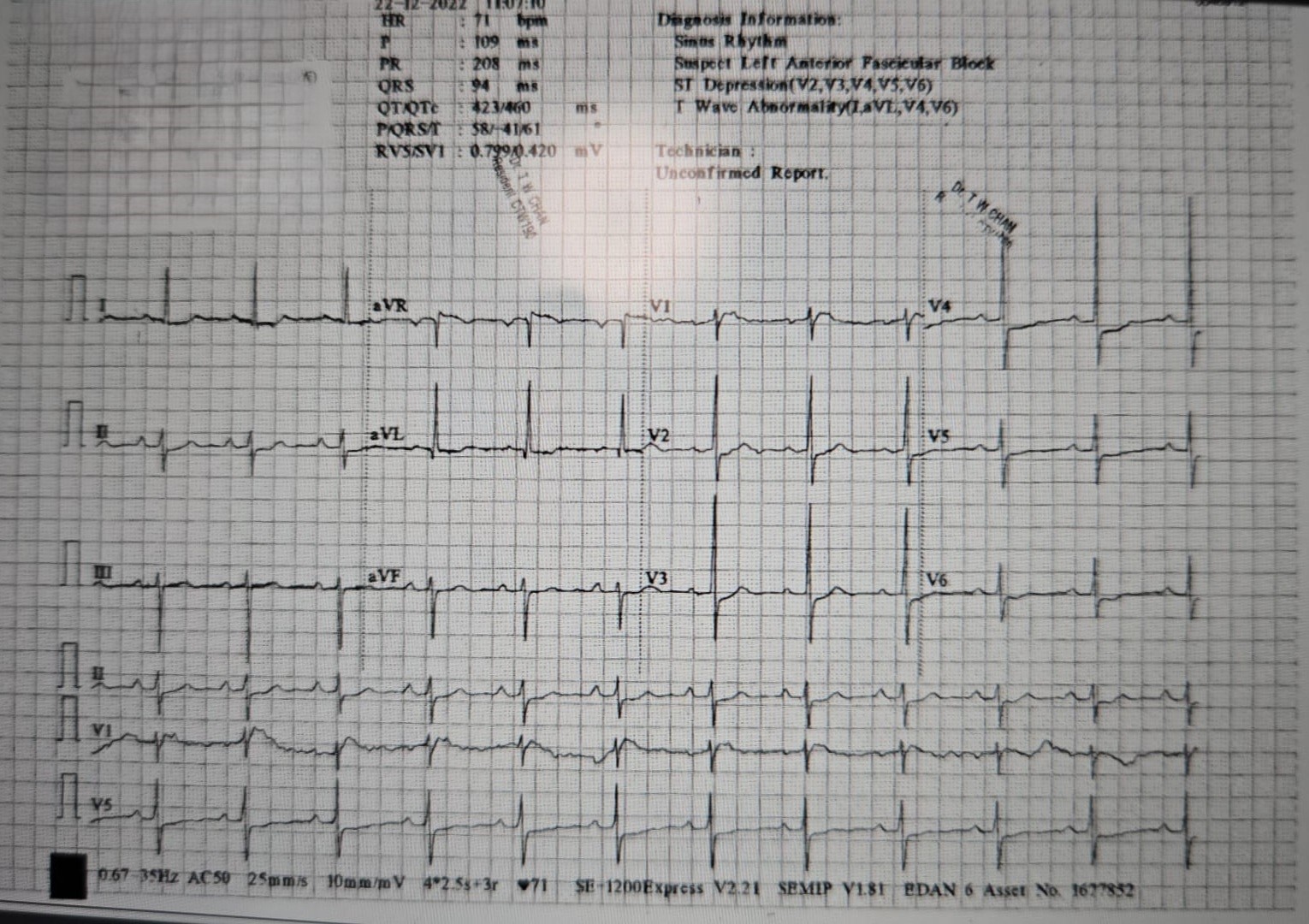
The electrocardiogram at admission showed diffuse ST depression in leads V2-V6. Echocardiogram showed left ventricular ejection fraction was 60% and no obvious regional wall motion abnormalities and significant valvular lesions. Peak Troponin I was 488 ng/L.
Relevant Catheterization Findings
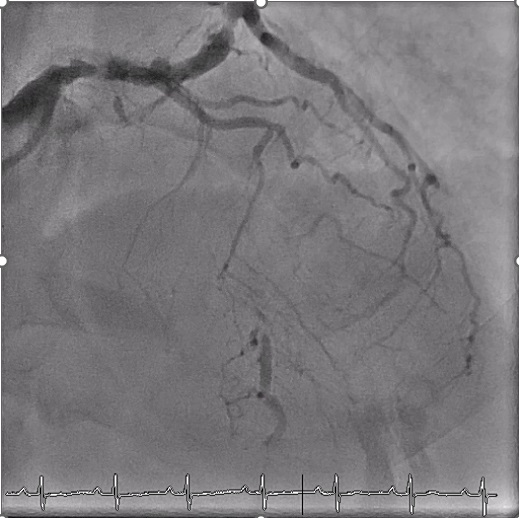
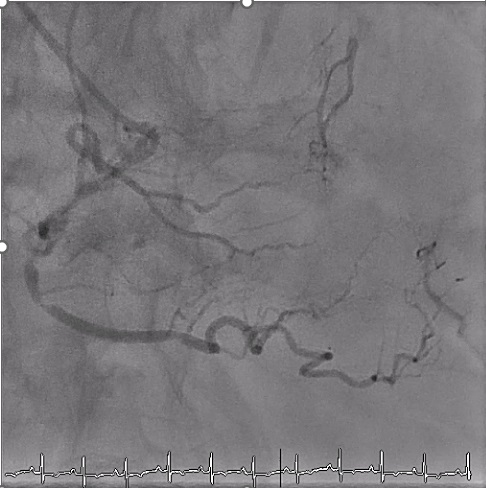
Coronary angiogram showed 90% stenosis in distal left main artery. Proximal left anterior descending artery (LAD) had chronic total occlusion (CTO) lesions. Proximal left circumflex artery (LCX) had 90% stenosis. Middle LCX had CTO lesions with 70% stenosis in obtuse marginal branch. Right coronary artery (RCA) was non-dominant and small. Middle RCA showed 90% stenosis. Collaterals was seen from RCA to LAD and LCX.

Interventional Management
Procedural Step
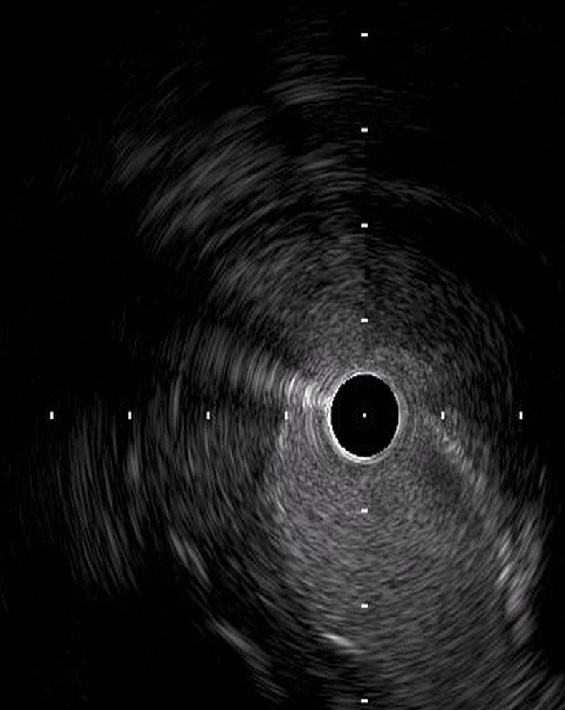
The case was discussed with cardiothoracic surgery (CTS) team who insisted on IABP insertion prior to CABG. IABP insertion failed due to extremely tortuous aorta. CTS team then turned down the patient for surgery due to high procedure risk. After a detailed discussion with patient and his relatives about all possible procedural risk, they agreed for high risk PCI. As the RCA is small and there is high risk of compromising the collaterals to the left coronary arteries, the team decided to attempt PCI to LM/LCX/OM. The ramus, LCX and OM was wired respectively. OM was crossed with a microcatheter. Proximal LCX was dilated with a SC balloon 2.0/15. Intravascular Ultrasound (IVUS) was used to identify the stump of the mLCX CTO. mLCX CTO was then crossed with Gaia 2 wire and Turnpike LP microcatheter. The m-dLCX was pre-dilated with NC Sapphire 0.85/10. OM was stented with 3.0/28 DES. OM was post dilated with NC 3.0 balloon. Proximal part of the OM DES was crushed with NC 3.0 balloon. M-dLCX was stented with 3.5/28 DES. OM was then rewired and first kissing balloon inflation (KBI) was done. LM to mLCX was stented with 4.5/22 DES. POT to LM was done with NC 4.5 balloon. The patient complained of chest pain at the moment and coronary angiogram showed jailing of the ramus. The ramus was rewired with a double lumen catheter and flow was regained. The OM was rewired again and second KBI was done. Final angiograms and IVUS showed good stent expansion, apposition and no complications.


Case Summary
The case illustrates the challenging decisions we face in the management advanced age CHIP cases. It also showed that intravascular ultrasound was useful in identify the stump of chronic total occlusion lesion. It also helps to rewire the jailed vessel.