
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-038
Rotational Atherectomy After Recanalization of Chronic Total Occlusion of the Right Coronary Artery
By Alexandr Shlykov, Alexey Sozykin, Emelyanov Pavel, Lyudmila Ulyanova, Chingis Delikov, Nataliya Novikova, Igor Lozovskii
Presenter
Lyudmila Ulyanova
Authors
Alexandr Shlykov1, Alexey Sozykin1, Emelyanov Pavel1, Lyudmila Ulyanova1, Chingis Delikov1, Nataliya Novikova1, Igor Lozovskii1
Affiliation
Petrovsky National Research Center of Surgery, Russian Federation1,
View Study Report
TCTAP C-038
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Rotational Atherectomy After Recanalization of Chronic Total Occlusion of the Right Coronary Artery
Alexandr Shlykov1, Alexey Sozykin1, Emelyanov Pavel1, Lyudmila Ulyanova1, Chingis Delikov1, Nataliya Novikova1, Igor Lozovskii1
Petrovsky National Research Center of Surgery, Russian Federation1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
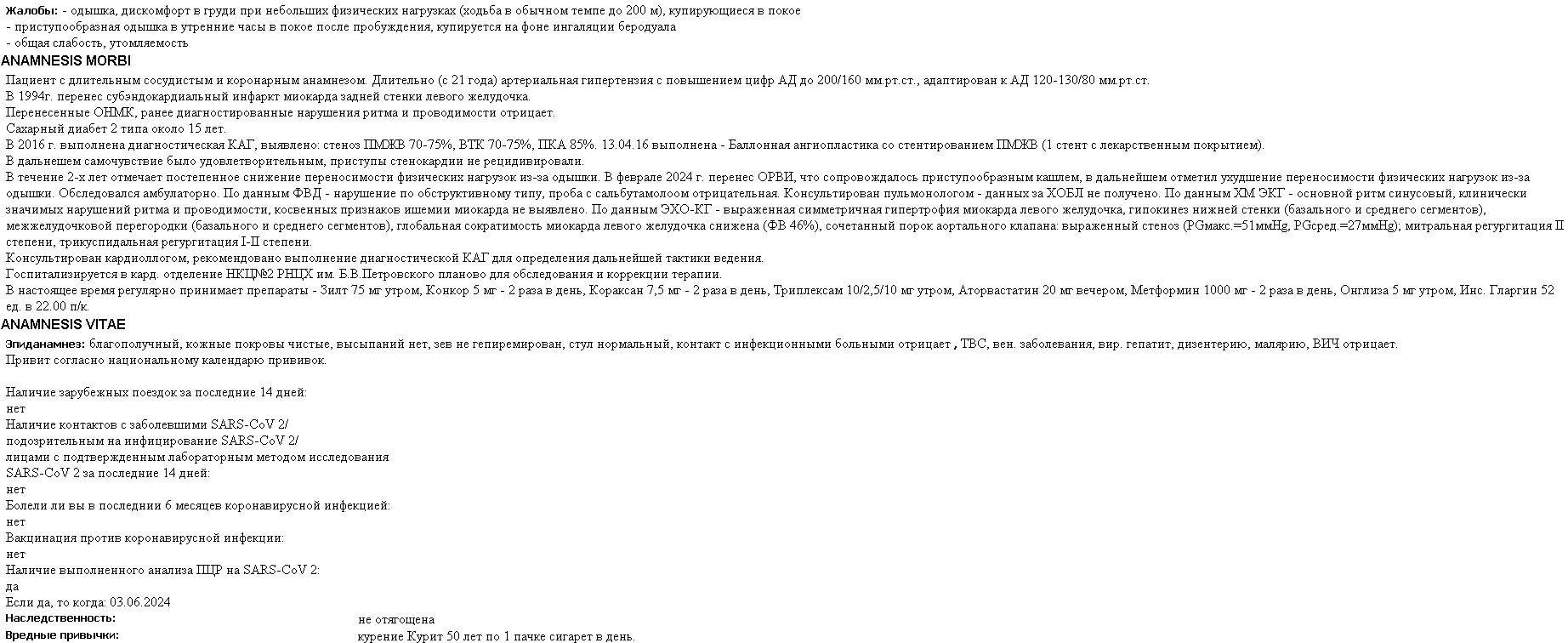
Male 62 years old. M iyocardial infarction 1994. Angina pectoris 2012 ye. Hypertension. Diabetes mellitus.
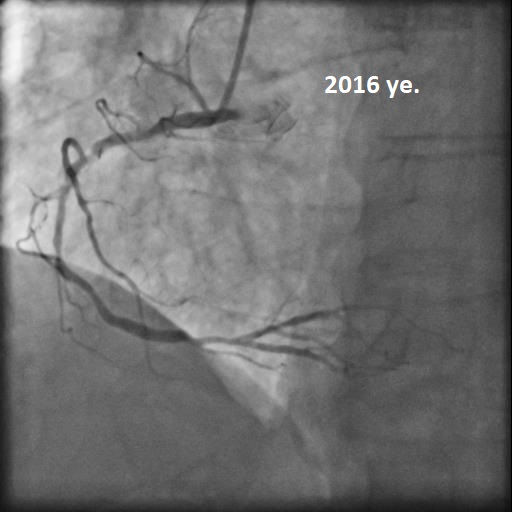
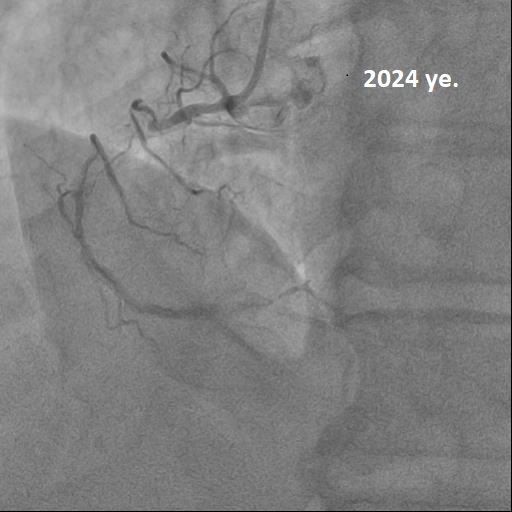
Coronary stenting of the anterior descending artery 2016 ye. In 2024 ye., after suffering from acute respiratory viral infection, he noted a deterioration in exercise tolerance due to shortness of breath.
The stress test is not informative (severe shortness of breath).
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Chronic occlusion of the right coronary artery
Interventional Management
Procedural Step
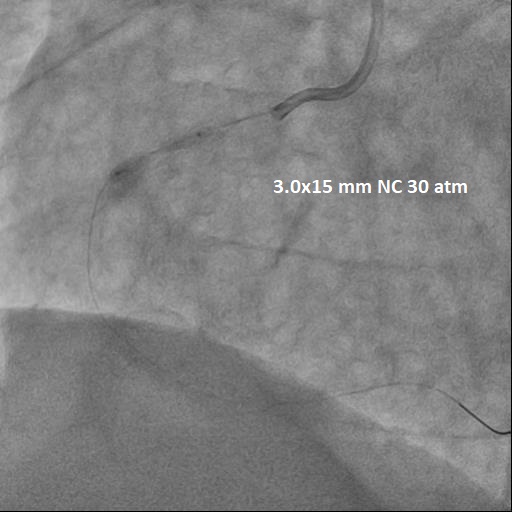
A guidecatheter is installed at the ostium of the RCA. Recanalization of the RCA was performed using coronary guidewire of varying stiffness using a microcatheter.


Case Summary
A device for performing rotational atherectomy is necessary to perform complex coronary interventions.