Coronary - Complex PCI - CTO
Turning Back to Move Forward: The Retrograde Approach Transforms the Landscape of Chronic Total Occlusion Interventions
Sigit Pratama Iustitia Nasruddin1, Yudi Her Oktaviono2
RSUD. Dr. H. Abdul Moeloek Hospital, Indonesia1, RSUD Dr. Soetomo, Indonesia2,
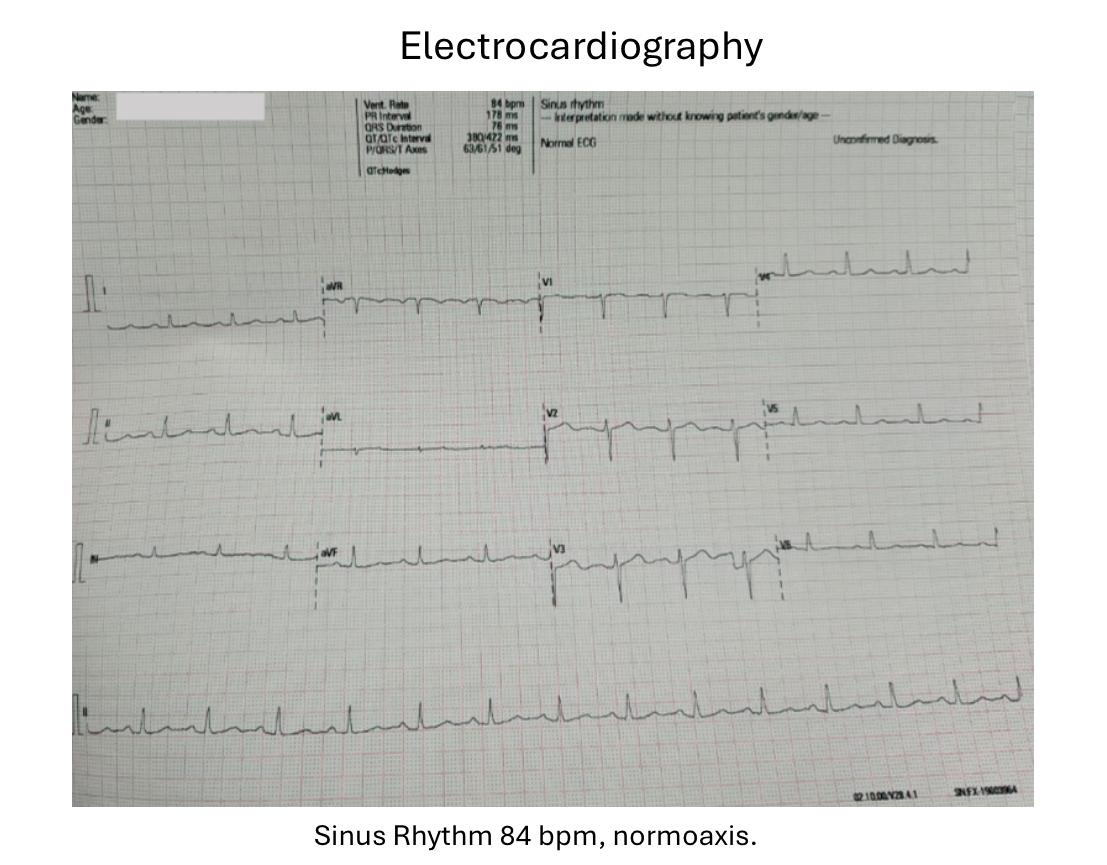
A 59-year-old female with hypertension and type 2 diabetes presented with exertional chest pain since six month ago. The pani often triggered by physical activity, stress, or heavy meals, and relieved by rest or nitroglycerin.
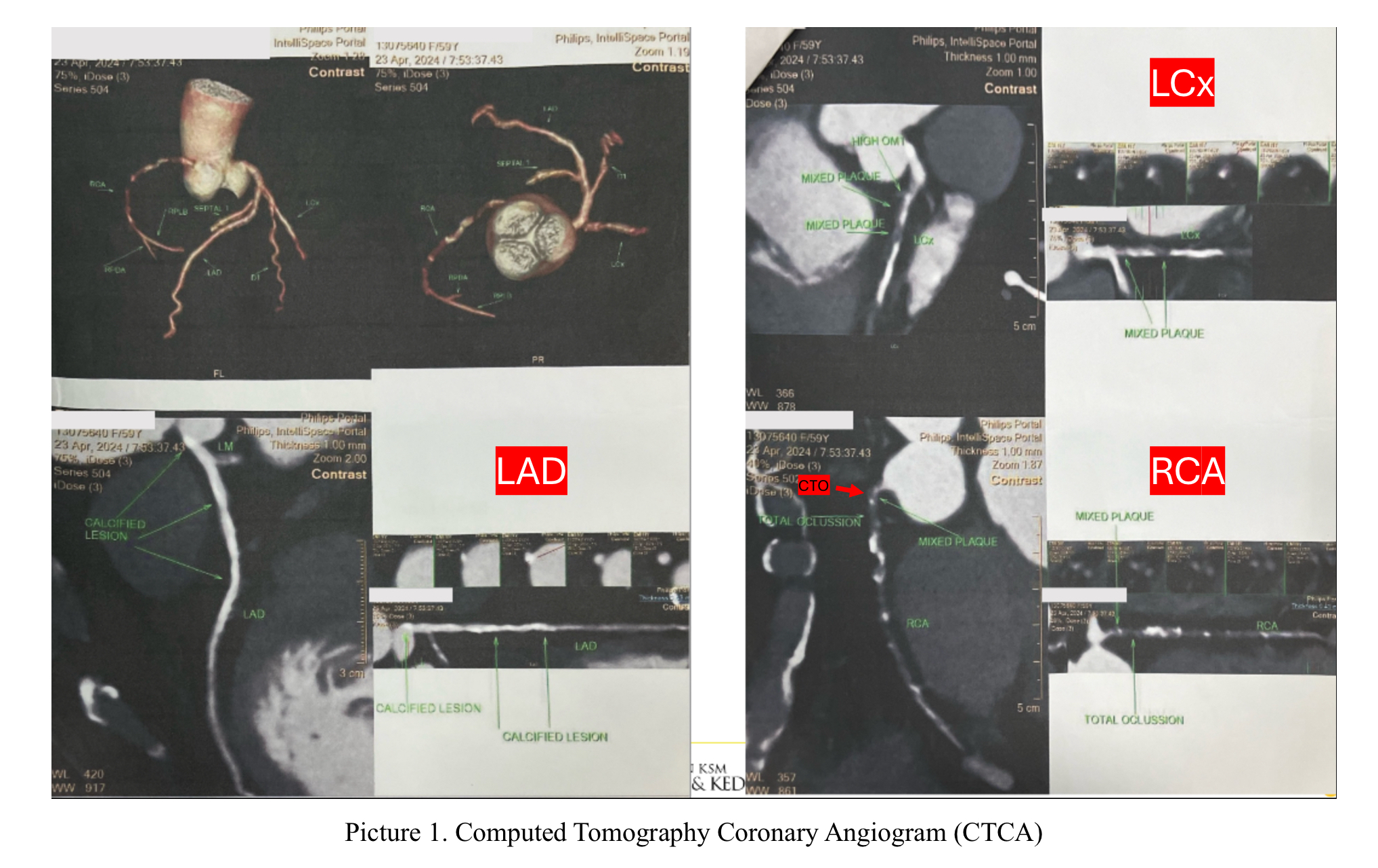
CTCA revealed Left Main: There is calcified plaque without luminal stenosis. LAD: There is calcified plaque with mild stenosis 30% at proximal. LCx: There is mixed plaque with severe stenosis (70-90%) at osteal. There is mixed plaque with critical stenosis at proximal. RCA: There is calcified plaque with severe stenosis (>80%) at osteal. There is total occlusion at proximal. There is no luminal stenosis at mid and distal RCA. Conclusion CAD Double Vessel Diseases with CAD-RADS 5/P4.
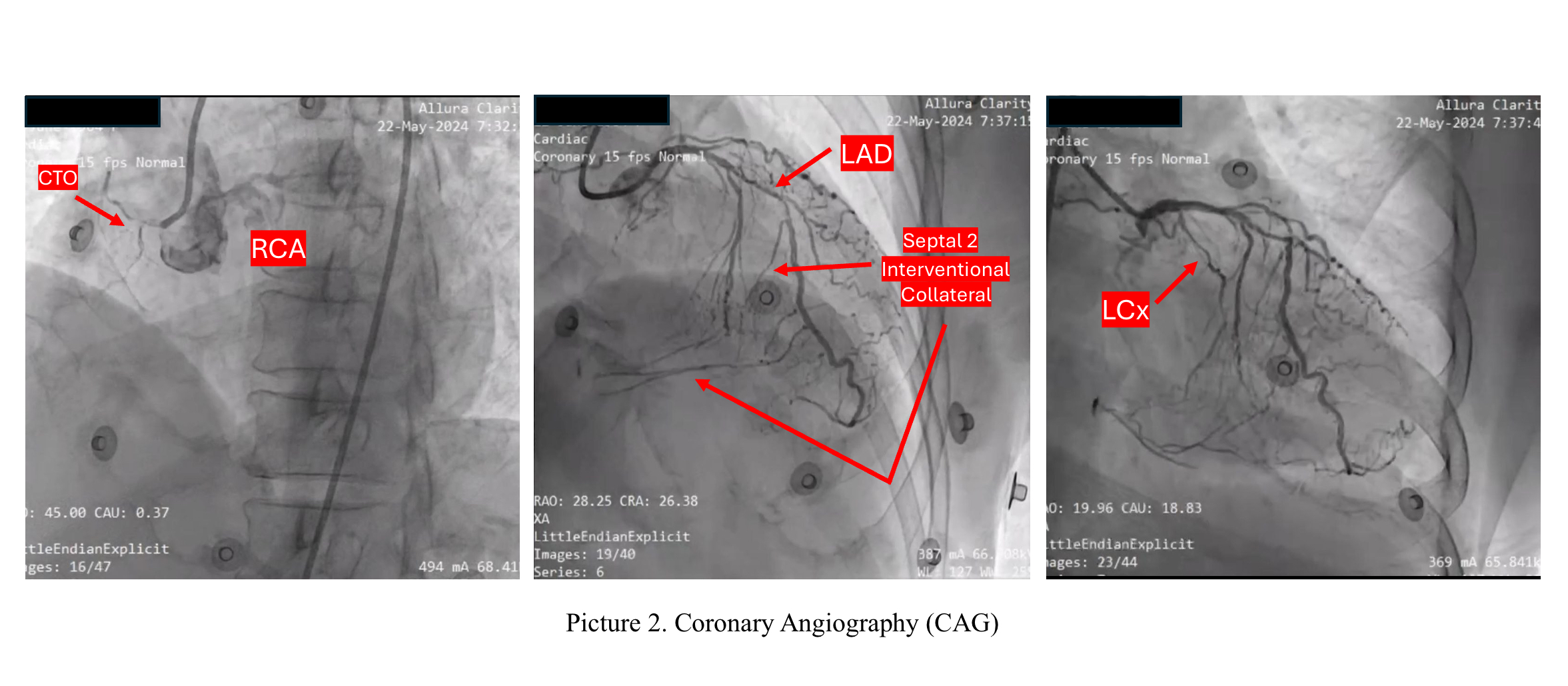
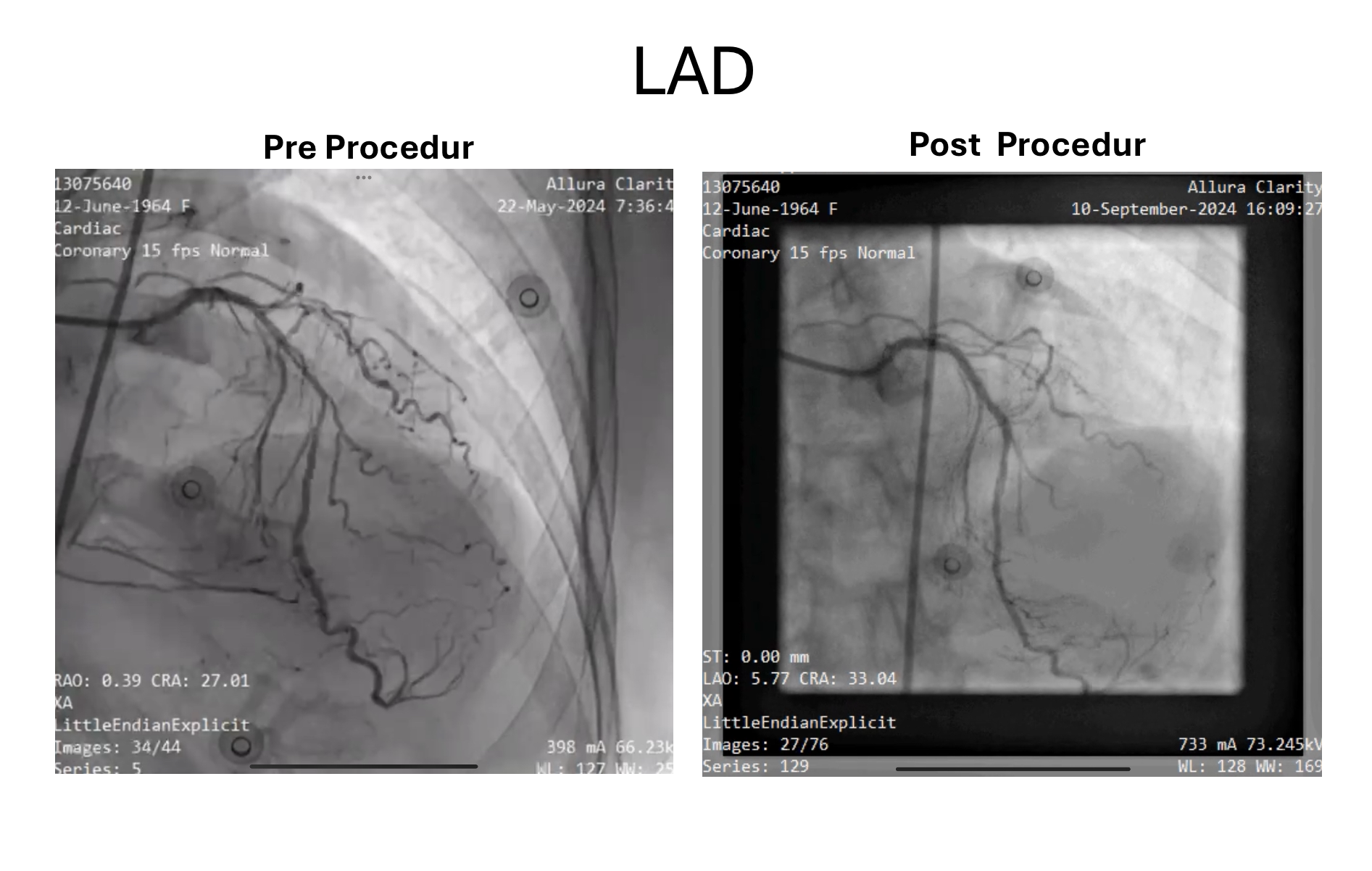
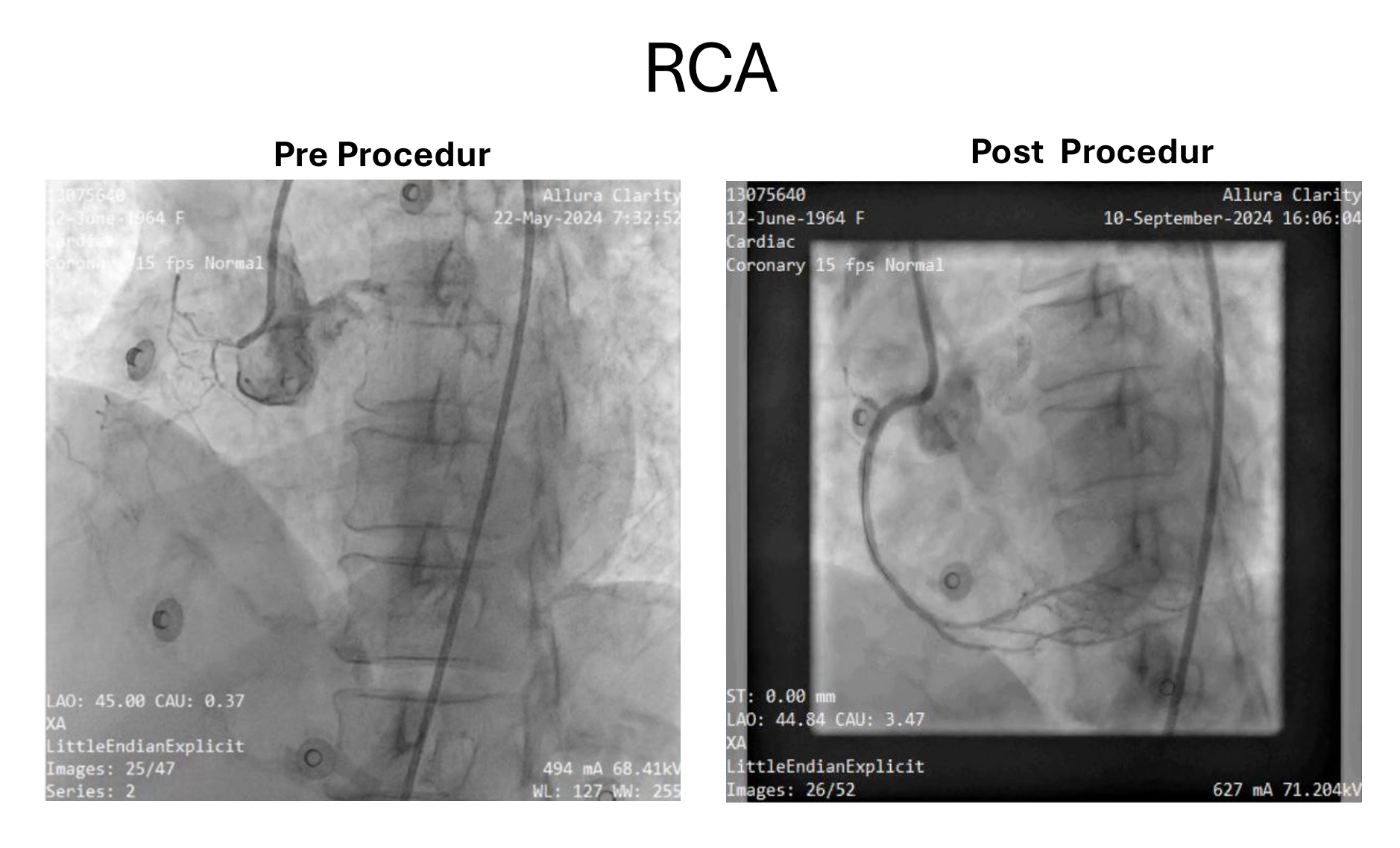
CAG showed 90% stenosis of the LAD artery, 80% stenosis of the distal LCx but small vessel, and chronic total occlusion (CTO) of the proximal right coronary artery, with good collateral circulation from the septal LAD to the distal RCA. The patient declined coronary artery bypass grafting (CABG) and opted for percutaneous coronary intervention (PCI). An antegrade PCI to the LAD was planned, followed by a retrograde approach for the RCA CTO, given its high degree of difficulty (JCTO score 3).
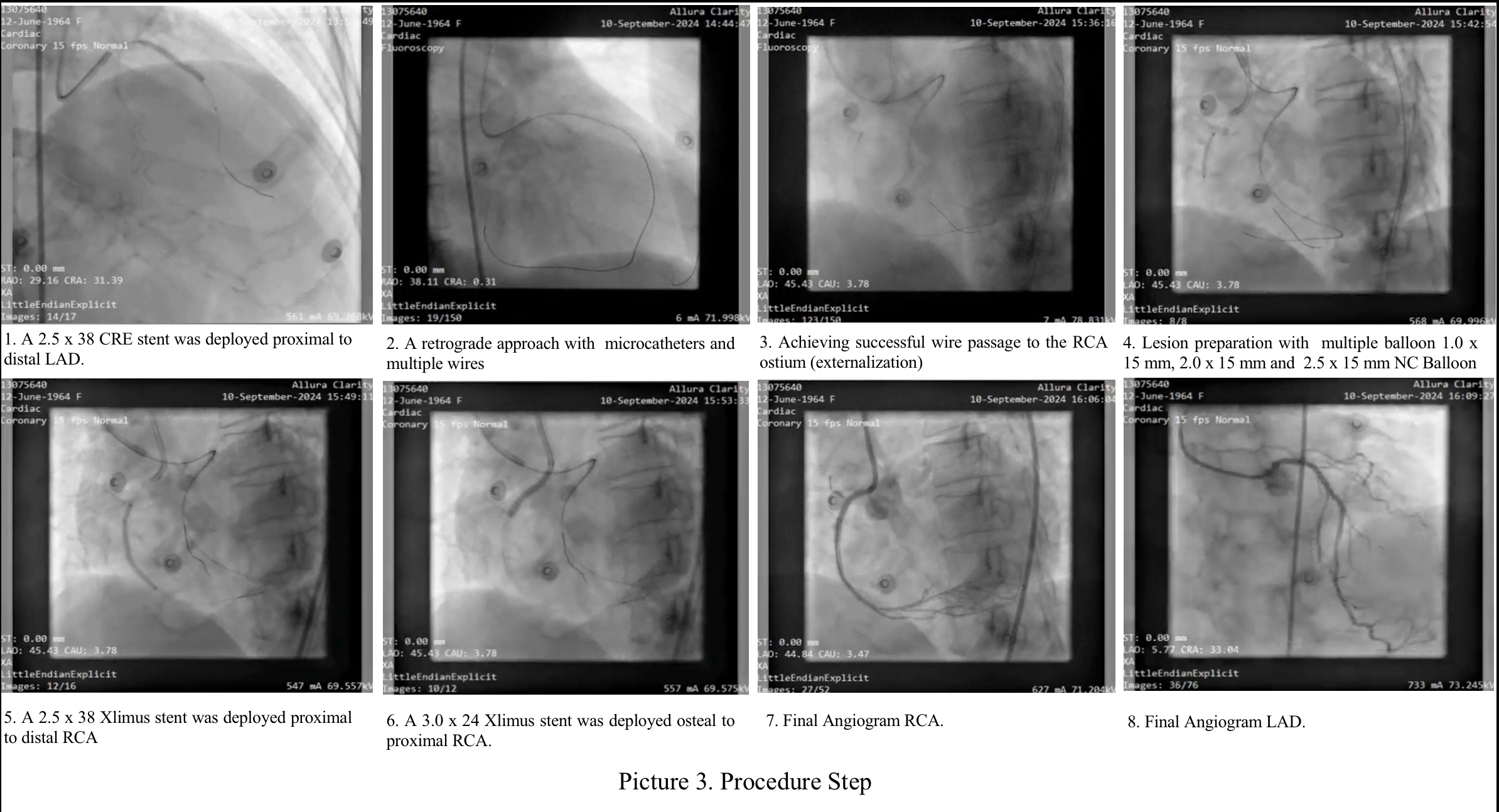
The procedure begins with the placement of a BL 3.0 7F guide catheter through the left femoral artery to connect the LMCA. A Sion Blue wire is advanced to the distal LAD, followed by predilation with a Sapphire II Pro 2.0 x 20 mm balloon. A CRE 8 2.5 x 38 mm stent is placed from the proximal to the distal LAD. For RCA CTO, a retrograde approach from the septal LAD is used. Microcatheters, including Caravel, and several wires ( Asahi Suoh 03, Fielder XT-R and Gladius EX14) are used to access the RCA until successful. A JR 4.0 7F guide catheter is inserted through the right femoral artery, ULTIMATEbros 3 wire and Corsair Pro microcatheter were advanced to the proximal RCA, followed by sequential predilation with a 1.0 x 15 mm Sapphire II Pro balloon and escalation with a 2.0 x 15 mm in the proximal to mid RCA. After removing the Corsair Pro microcatheter, a Guidezilla II guide extension catheter was inserted, followed by further balloon escalation with a 2.5 x 15 mm NC Experience balloon. Wire externalization was achieved with an RG3 wire, allowing placement of a 2.5 x 38 mm stent from the middle to the distal RCA and a 3.0 x 24 mm Xlimus stent from the ostium to the middle RCA. Kissing balloon inflation was performed to address residual stenosis in the right posterior descending (RPDA) and right posterolateral (RPL) branches. The final results showed TIMI grade 3 flow with no residual stenosis or complications, successfully restoring coronary blood flow.
Successful recanalization of coronary chronic total occlusions (CTO) can yield significant clinical benefits but remains challenging, particularly due to difficulties in advancing a guidewire across the occlusion. The retrograde approach has represented a paradigm shift in CTO PCI and is now an essential component of contemporary CTO PCI techniques. While retrograde CTO PCI improves success rates, it also presents a higher risk of complications and should therefore be reserved for use by experienced operators in specialized centers.
