
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-221
Cardiac Renaissance: TAVI Implantation During Asystole
By Liudmila Ulyanova, Alexsei Sozykin, Alexandr Shlykov, Novikona Natalia, Emelyanov Pavel, Delikov Chingiz, Igor Lozovsky
Presenter
Liudmila Ulyanova
Authors
Liudmila Ulyanova1, Alexsei Sozykin1, Alexandr Shlykov1, Novikona Natalia1, Emelyanov Pavel1, Delikov Chingiz1, Igor Lozovsky1
Affiliation
Petrovsky National Research Center of Surgery, Russian Federation1,
View Study Report
TCTAP C-221
Structural - Other Structural Interventions
Cardiac Renaissance: TAVI Implantation During Asystole
Liudmila Ulyanova1, Alexsei Sozykin1, Alexandr Shlykov1, Novikona Natalia1, Emelyanov Pavel1, Delikov Chingiz1, Igor Lozovsky1
Petrovsky National Research Center of Surgery, Russian Federation1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
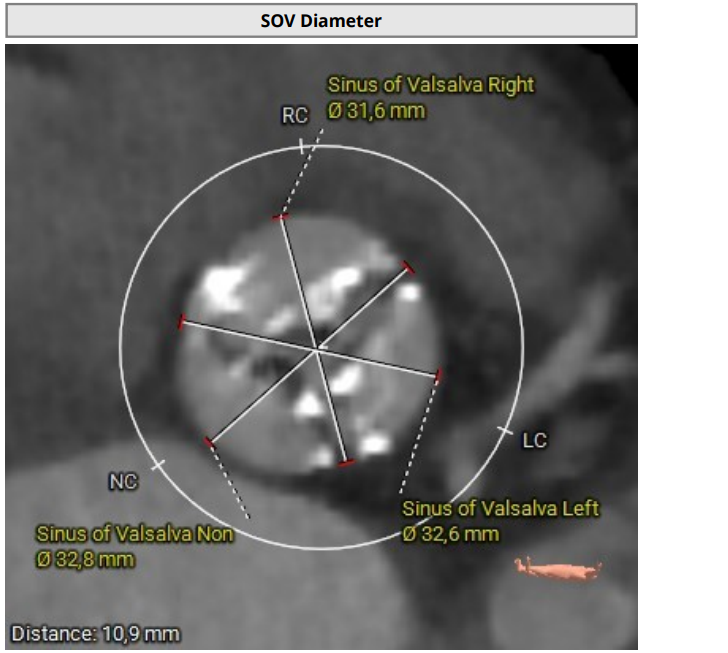
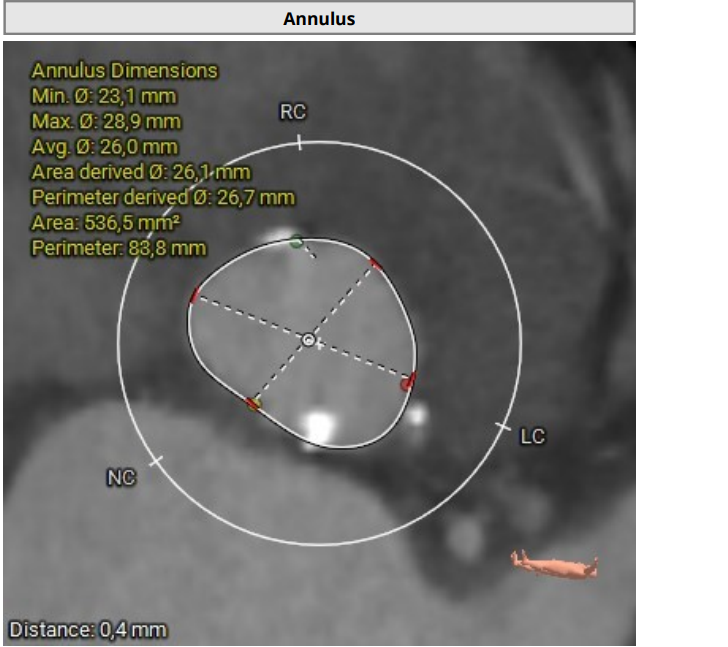
Since 2023 - frequent hospitalizations due to attacks of chest pain, attacks of nocturnal asthma. According to echocardiography - EF-52%. AV leaflet opening 0.5 cm. Prominent calcification of the aortic valve and fibrous ring. V-5.9 m/s, PGmax-140 mmHg, PGmean-88 mmHg, S-0,5 cm2. Aortic regurgitation grade II. Mitral regurgitation grade II-III. No zones of local contractility disturbance. Consulted with a cardiac surgeon, surgical correction of aortic defect was recommended.
Relevant Test Results Prior to Catheterization
Clinical blood test: RBC – 4,4 10 in 12 tbsp. / l; HGB - 135 g / l; MCV – 91,3 cubic meters; PLT - 260 10 in 9 st. / l; MPV – 8.7 cubic meters; Leukocytes – 6.7 10 in 9 tbsp. / l; Segmented neutrophils,% - 73.9%; Lymphocytes – 15,9%; Monocytes - 8.5%; Eosinophils - 0.8%; Basophils - 0.8%; Erythrocyte sedimentation rate - 28 mm / h;Biochemical blood test: Potassium – 4,13 mmol / l; Glucose – 5,7 mmol / L; GFR (MDRD) M – 62,9 ml / min / 1.73m2; Serum creatinine – 81,8μmol / l.
Relevant Catheterization Findings
Interventional Management
Procedural Step
The rightsubclavian vein was punctured. A 6F intraducer was inserted. The endocardialelectrode for temporary cardiac stimulation was placed in the right ventricularcavity. The left radial artery was punctured. A 6F intraducer was placed, andan invasive pressure line was connected. The left common femoral artery waspunctured. The 6F intraducer is inserted. Pigtail 6 F diagnostic catheter isinserted into the non-coronary sinus. Puncture of the right common femoralartery was performed. Two intravascular sutures were placed using the Pro Glidepre-stitching technique. The 12F intraducer was placed in the lumen of the rightfemoral artery. The Confida wire wasguided into the left ventricular cavity. Aortic valve valvuloplasty wasperformed using balloon catheters 20.0-40.0 mm, 25.0-40.0 mm. Asystole wasregistered on ECG and resuscitative measures were started. During indirectheart massage, endovascular prosthesis Portico - 29mm was implanted in aorticposition. At the control aortography, the aortic valve prosthesis is optimallyspread out.



Case Summary
Inpatients with critical aortic stenosis (combined with regurgitation), afterballoon predilatation, there is a high probability of developing total LVfailure. Radipimplantation of TAVI within 1-2 minutes is required to prevent a fatal outcome.Even in asystole. Thecurrent Guidelines don’t contain any algorithms for actions in such cases. There’reonly proctor recommendations from manufacturing companies. Such an algorithm is needed in Guidelines.