
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-205
The Regret That We Accepted: Managing High-Risk Multivessel Coronary Artery Disease and Severe Aortic Stenosis in a Patient With a Porcelain Aorta
By Sunanto Ng, Teguh Santoso
Presenter
Sunanto Ng
Authors
Sunanto Ng1, Teguh Santoso2
Affiliation
University Pelita Harapan, Indonesia1, Medistra Hospital, Indonesia2,
View Study Report
TCTAP C-205
Structural - Aortic Valve Intervention - Complex TAVR
The Regret That We Accepted: Managing High-Risk Multivessel Coronary Artery Disease and Severe Aortic Stenosis in a Patient With a Porcelain Aorta
Sunanto Ng1, Teguh Santoso2
University Pelita Harapan, Indonesia1, Medistra Hospital, Indonesia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
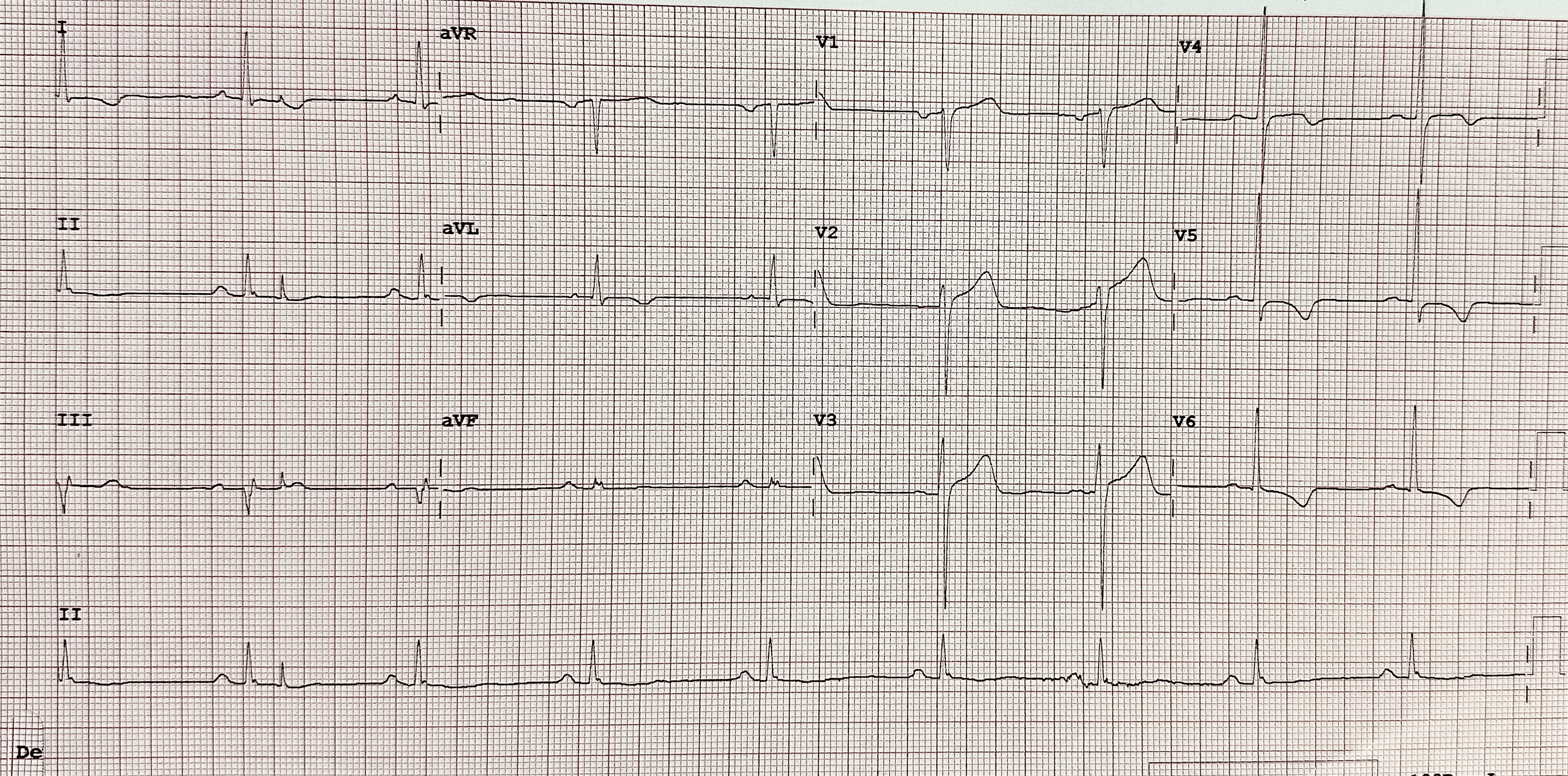
A 76-year-old male presented with worsening angina over the past year. He had multivessel coronary artery disease (CAD) with a prior percutaneous coronary intervention (PCI) in 2004, severe aortic stenosis (AS), and multiple comorbidities, including diabetes mellitus, hypertension, and chronic obstructive pulmonary disease (COPD) and chronic kidney failure (eGFR 46 mL/min/1.73m²). Physical examination revealed an ejection systolic murmur. ECG revealed left ventricular hypertrophy.
Relevant Test Results Prior to Catheterization
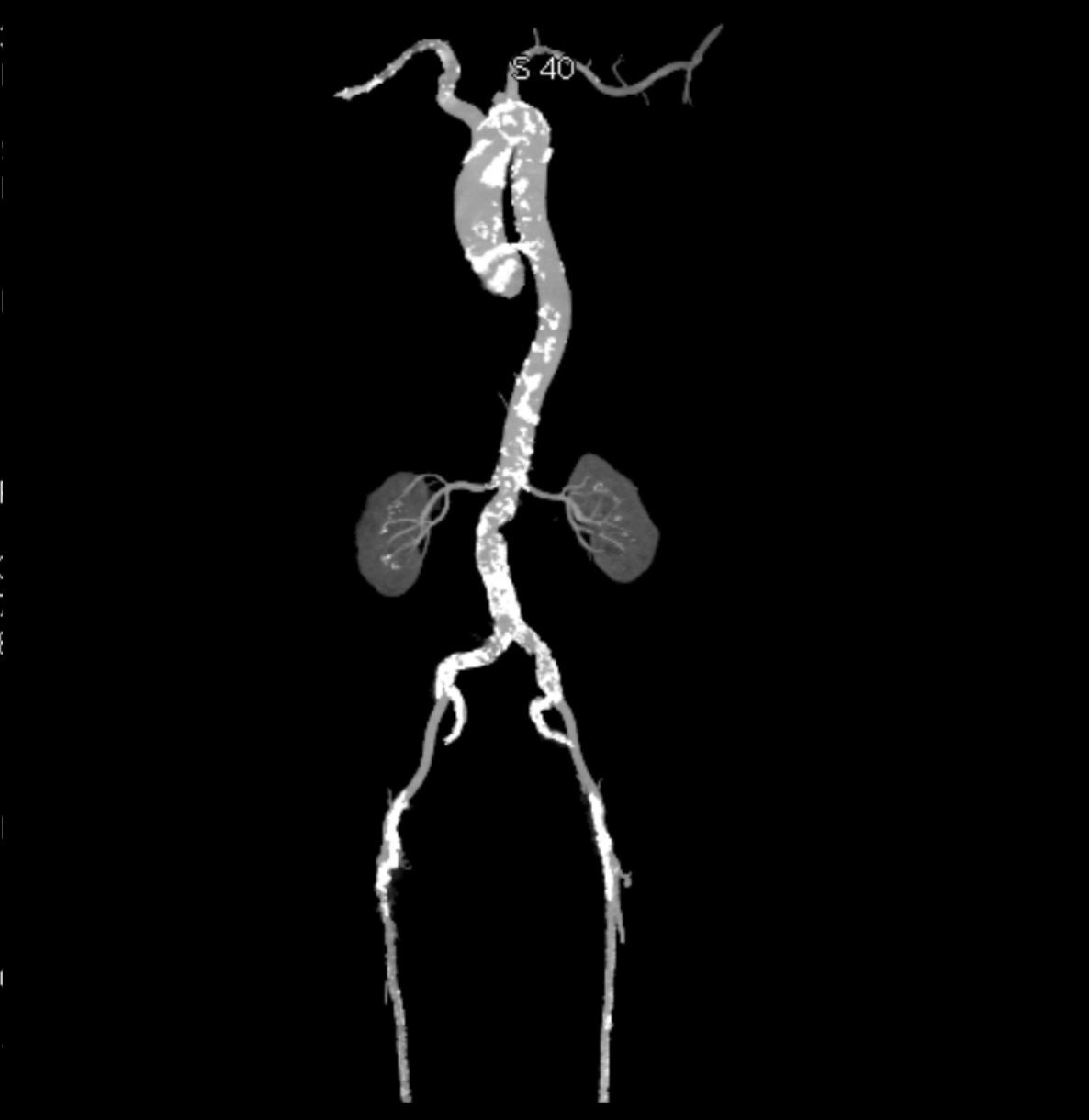
Echocardiography confirmed severe aortic stenosis with a tricuspid aortic valve (aortic valve area 0.9 cm², peak gradient 42 mmHg, mean gradient 25 mmHg) and mildly reduced left ventricular function (LVEF 45%). CT angiography demonstrated extensive calcification of the thoracic and abdominal aorta, severe stenosis of the right superficial femoral artery, and significant stenosis at the ostia of both renal arteries. The aortic valve showed severe calcification, with an Agatston score of 3017.
Relevant Catheterization Findings
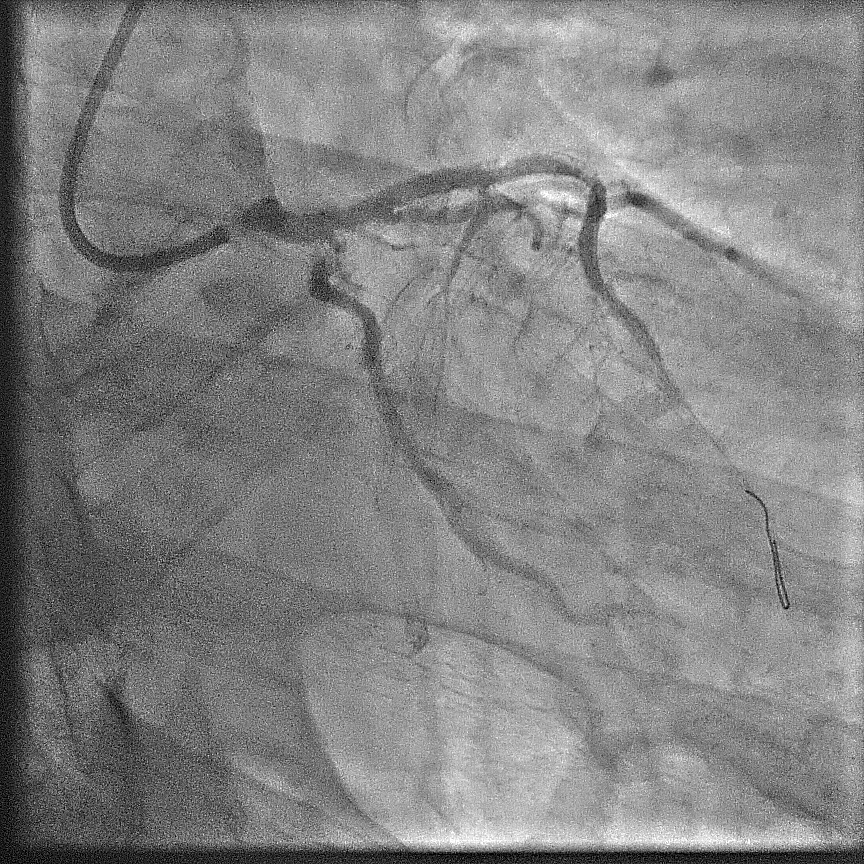
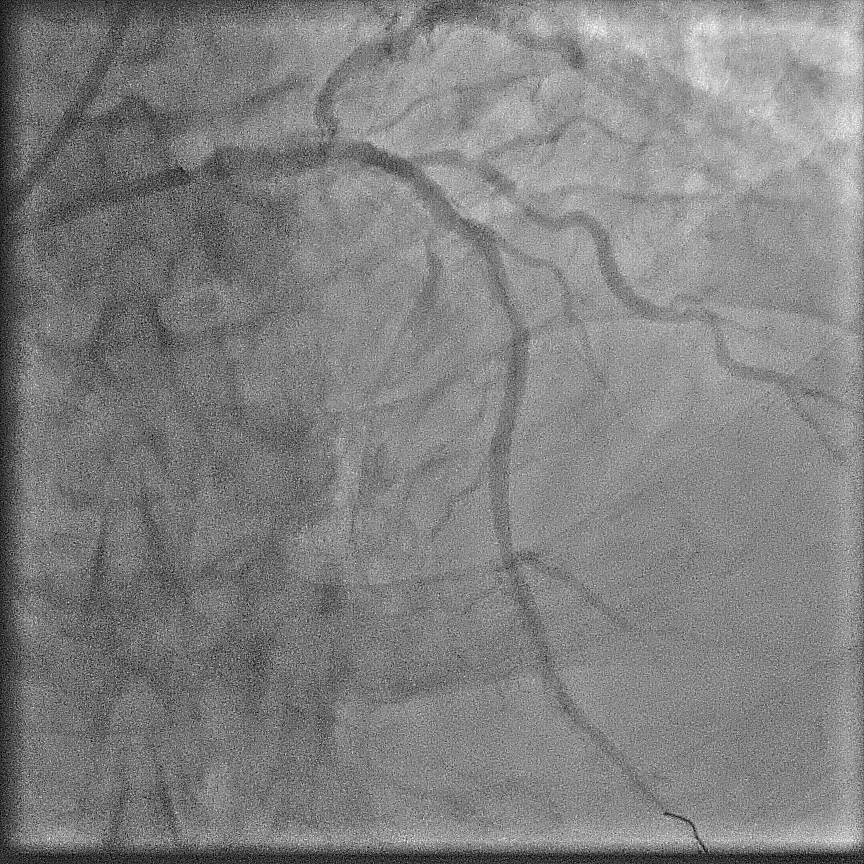
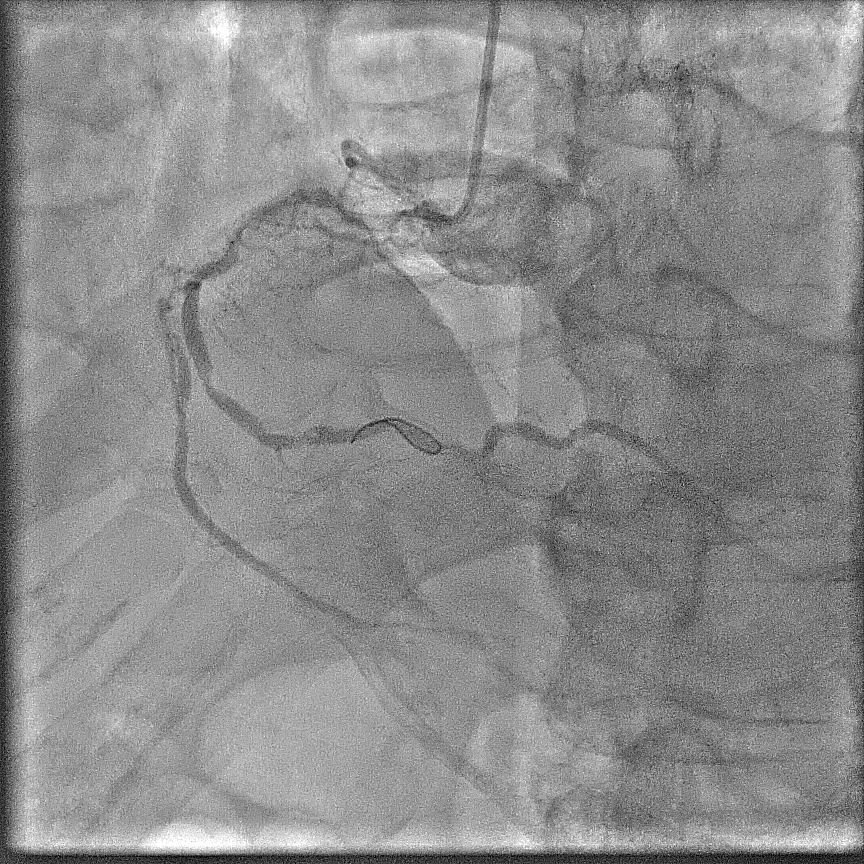
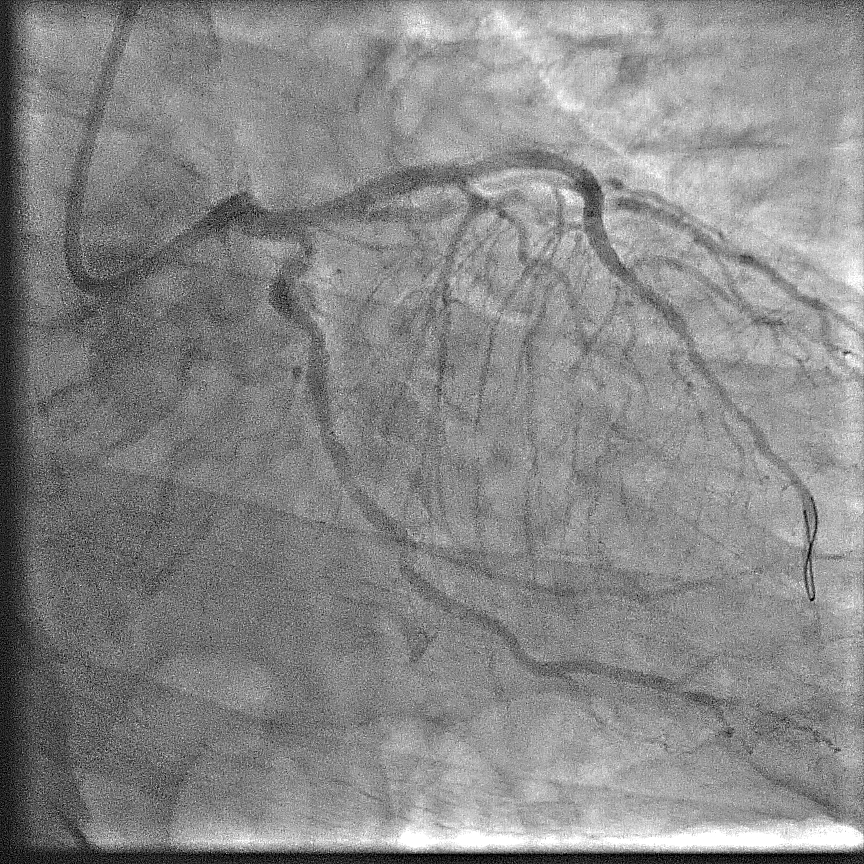
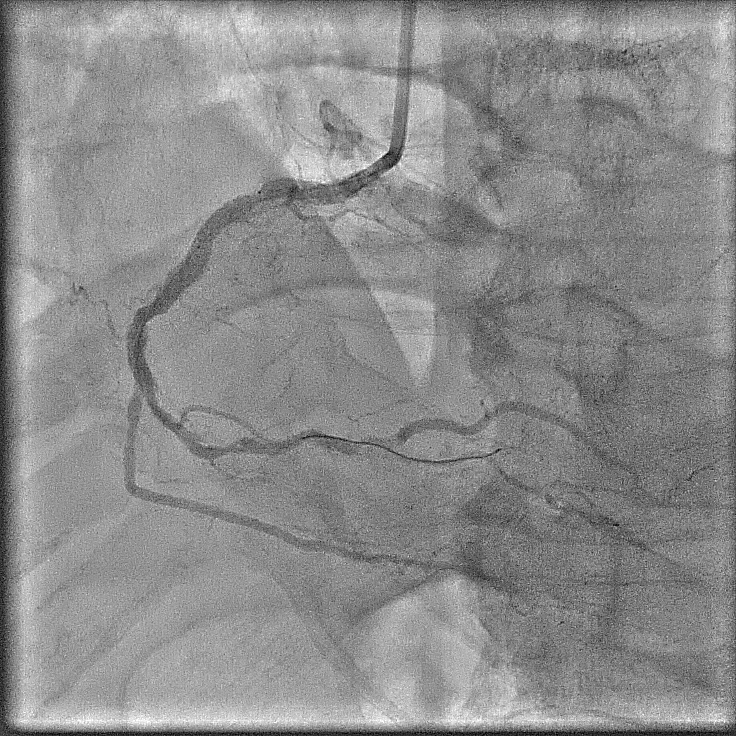
Angiography showed extensive calcification in the left and right coronary arteries, with severe stenosis at the left main ostium, severe in-stent restenosis at mid LAD, and severe, tortuous stenosis at the ostium and proximal LCx. The RCA was severely diffuse diseased with heavy calcification. The SYNTAX score was 58; BCIS CHIP score 7/13 - a very high risk and complex anatomy for PCI. STS surgery score risk for mortality was 3%; mortality and morbidity 18%.
Interventional Management
Procedural Step
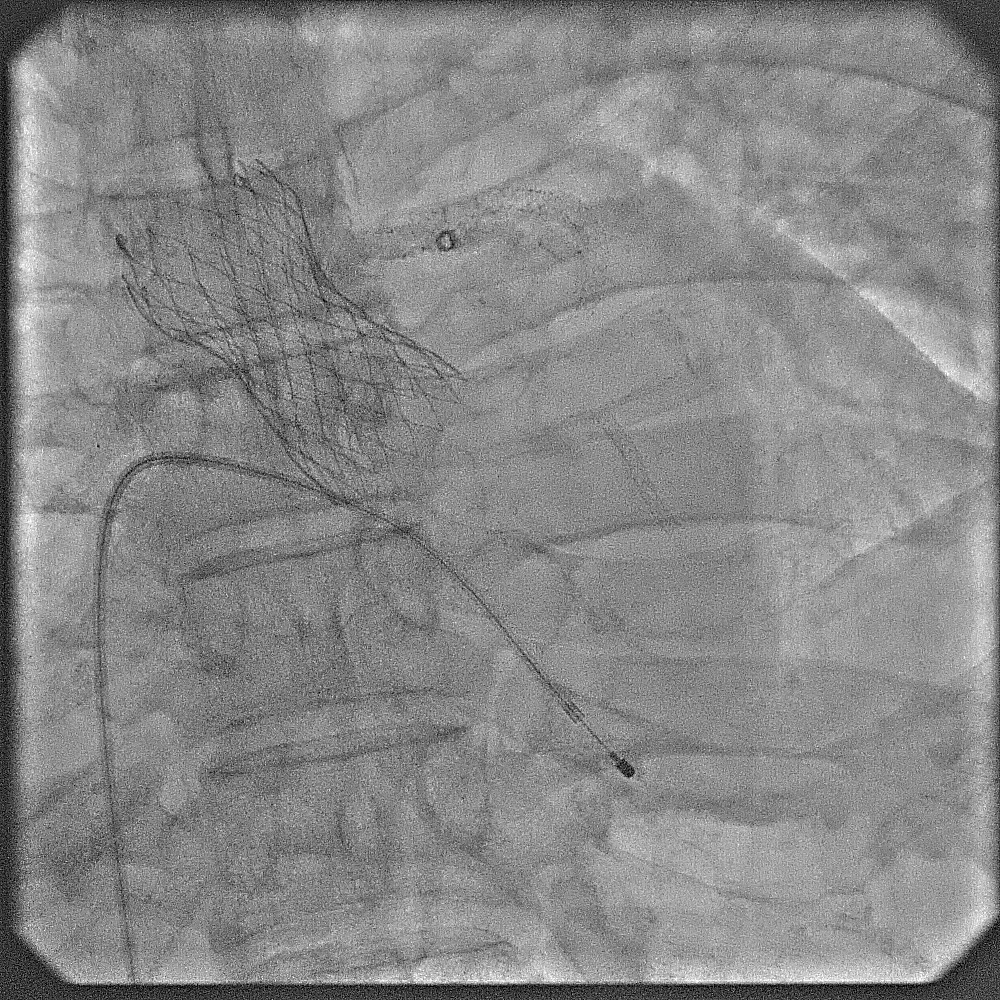
The case was referred to cardiac surgeon. Due to extensive calcification of the aorta, surgery was deemed highly challenging. With surgery declined, a staged procedure of PCI and transcatheter aortic valve replacement (TAVR) was planned. Throughout, contrast use was minimized to reduce renal injury.First Procedure: Initial PCI targeted the left coronary system. Pre-dilation was performed at left main ostium, followed by at the most obstructive lesion in the LCx to reduce the risk of ischemia in subsequent interventions. The mid-LAD was treated with a drug-eluting balloon (DEB), followed by the LCx with DEB. Finally, the left main ostium was stented with a drug-eluting stent (DES), achieving a favourable outcome. Total contrast volume used was 28 mL.Second Procedure: The next day, PCI was performed on the RCA. Despite the challenging ostial lesion, positioning of the guiding catheter (AL1) was successful. Balloon pre-dilation and placement of two DESs in the proximal RCA achieved satisfactory result. Total contrast used was 31 mL. The patient experienced significant relief from angina following these interventions.One Month Later: TAVR was performed using an Evolut Pro+. Due to severe iliofemoral and aortic calcifications, device delivery was challenging. TAVR was ultimately succesful; peak aortic valve gradient was decreased from 50 mmHg to no residual gradient.
Case Summary
This case highlights the viability of PCI and TAVR as alternative treatments for high-risk patients with multivessel CAD, severe AS, and a porcelain aorta. Despite significant procedural challenges and high baseline risk, the patient achieved an excellent outcome, underscoring the importance of thorough risk assessment and advanced interventional techniques in managing complex cardiovascular cases.