
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-181
A Challenging Case Report: Massive Pulmonary Embolism and Triple Vessel Disease
By Brian Terence Flynn
Presenter
Brian Terence Flynn
Authors
Brian Terence Flynn1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-181
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
A Challenging Case Report: Massive Pulmonary Embolism and Triple Vessel Disease
Brian Terence Flynn1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
We report a 60 year old gentleman with a history of hypertension, hyperlipidemia and diabetes mellitus who was admitted for Fournier gangrene and obstructive shock. Following surgery, a high-risk pulmonary embolism complicated his hospitalisation, necessitating a successful catheter-based endovascular thrombectomy with VA-ECMO support. Following recovery and a family conference, he underwent high-risk percutaneous coronary intervention (CHIP).
Relevant Test Results Prior to Catheterization
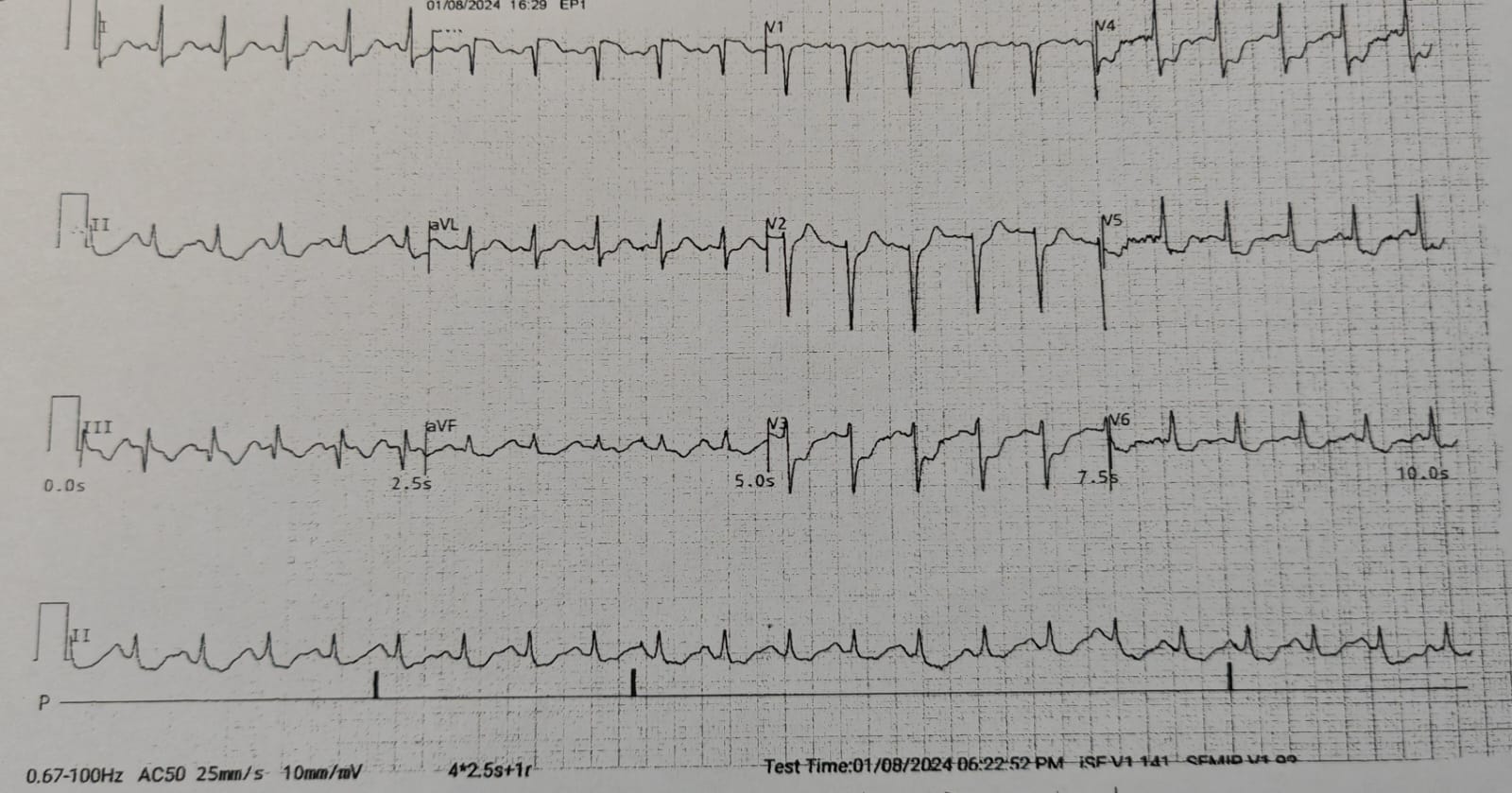
TnI : 8507 ng/LECG: SR STE aVR, diffuse ST depression
CT Pulmonary Angiogram: Massive emboli at main pulmonary trunk and bilateral pulmonary artery. Evidence of right heart strain with enlarged right ventricle and septal deviation.
Echocardiogram: Severely impaired LV systolic function, LVEF 34% by Simpson’s. Hypokinesia over basal to apical anterior and anteroseptal LV wall. LV diastolic dysfunction. Mildly calcified MV and tri-leaflet AV. Mild MR. Mild AR. No AS. Mild TR. No PHT (RVSP 30mmHg).
CT Pulmonary Angiogram: Massive emboli at main pulmonary trunk and bilateral pulmonary artery. Evidence of right heart strain with enlarged right ventricle and septal deviation.
Echocardiogram: Severely impaired LV systolic function, LVEF 34% by Simpson’s. Hypokinesia over basal to apical anterior and anteroseptal LV wall. LV diastolic dysfunction. Mildly calcified MV and tri-leaflet AV. Mild MR. Mild AR. No AS. Mild TR. No PHT (RVSP 30mmHg).
Relevant Catheterization Findings
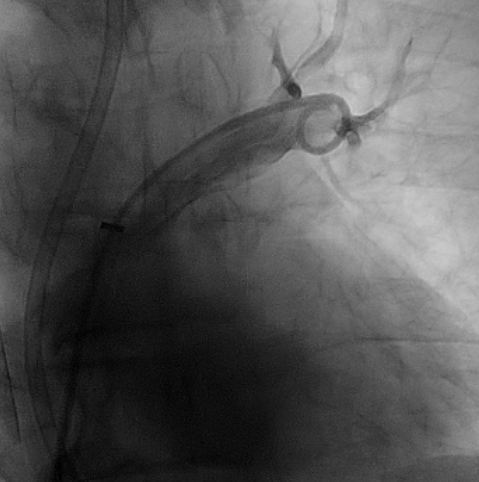
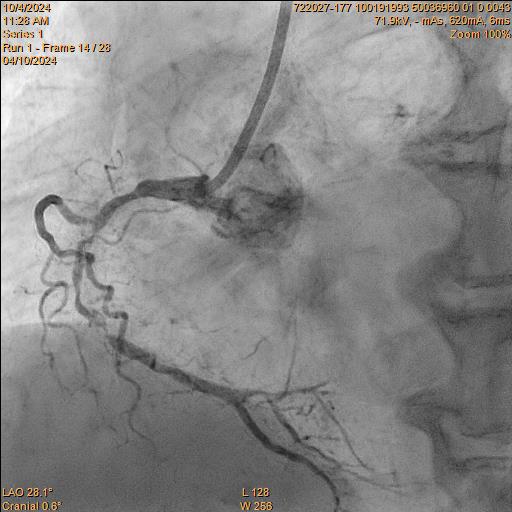
Pulmonary ArteriographyPA Pressure 55/26/36 mmHg. Pulmonary Arteriogram: Massive filling defect at main pulmonary trunk and bilateral pulmonary arteries (PA).Successful mechanical thrombectomy was performed under VA-ECMO Coronary AngiogramLMS: Mild diseaseLAD: Occluded from pLAD segment onward, retrograde from right systemLCx: Co-dominant, diffuse disease, critical stenosis at mLCxRCA: Co-dominant, mRCA critical stenosis, retrograde to LAD
Family conference: opt for high-risk PCI


Family conference: opt for high-risk PCI
Interventional Management
Procedural Step
Index ProcedureUnder VA-ECMO support (right internal jugular vein and right common femoral artery approach), successful mechanical thrombectomy was performed on the right and left PA with Lightning 12 Aspiration Catheter, clot separator and Silverway guidewire. Repeat PA angiogram showed flow restoration and improved PA pressure 31/18/23 mmHg.The patient subsequently stabilised, Coronary Angiogram and staged PCI was arranged.
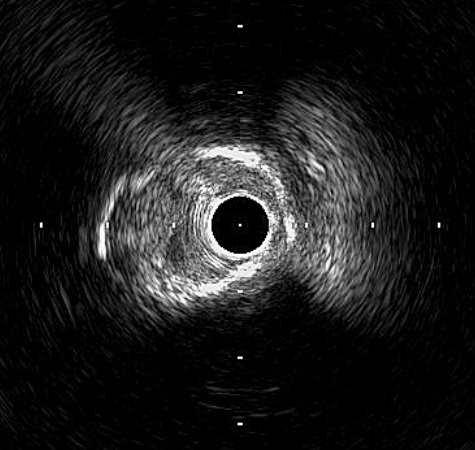
Intervention of RCA Right Coronary Artery was engaged with JR 7Fr Guiding Catheter. Lesion was successful wired with Fielder XT-R and was changed back to workhorse (NS Runthrough) wire. Sequential predilatation using 1.0/15 Sapphire, 1.5/15 Sapphire II Pro, and 2.25/15 Sapphire II Pro was then carried out with Guideplus II assistance; unfortunately, severe balloon underexpansion was noted. Rotational Atherectomy (RA) was attempted 1.25mm Burr for 2 passes at 180k rpm. Lesion was further prepared with 3.0/13 NSE Aperta and 3.0/10 NC Sapphire 24 under Intra-vascular ultrasound (IVUS) guidance before deploying overlapping 3.0/40 Orsiro Mission, 3.5/40 Orsiro Mission and 4.0/18 Orsiro Mission. Repeat IVUS after stent optimization showed stent underexpansion. Hence, intravascular lithrotripsy (IVL) was performed with Shockwave 3.5/12 for a total of 80 shocks, followed by 3.0/10 NC Sapphire stent optimization.
A later date was scheduled for staged PCI to the left system.
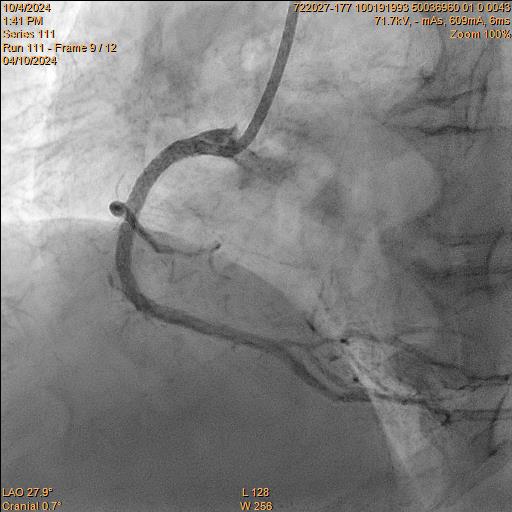
Intervention of RCA Right Coronary Artery was engaged with JR 7Fr Guiding Catheter. Lesion was successful wired with Fielder XT-R and was changed back to workhorse (NS Runthrough) wire. Sequential predilatation using 1.0/15 Sapphire, 1.5/15 Sapphire II Pro, and 2.25/15 Sapphire II Pro was then carried out with Guideplus II assistance; unfortunately, severe balloon underexpansion was noted. Rotational Atherectomy (RA) was attempted 1.25mm Burr for 2 passes at 180k rpm. Lesion was further prepared with 3.0/13 NSE Aperta and 3.0/10 NC Sapphire 24 under Intra-vascular ultrasound (IVUS) guidance before deploying overlapping 3.0/40 Orsiro Mission, 3.5/40 Orsiro Mission and 4.0/18 Orsiro Mission. Repeat IVUS after stent optimization showed stent underexpansion. Hence, intravascular lithrotripsy (IVL) was performed with Shockwave 3.5/12 for a total of 80 shocks, followed by 3.0/10 NC Sapphire stent optimization.
A later date was scheduled for staged PCI to the left system.
Case Summary
For patients in severe obstructive shock, endovascular thrombectomy is feasible in the setting of VA-ECMO support. This approach may benefit critically ill patients presenting with acute massive PE for whom mechanical thrombectomy is indicated. The association of PE with severe atherosclerosis has been well documented. Early diagnosis and prompt interventions are required to improve the clinical outcome in this subset population. We report the effective use of VA-ECMO during aspiration thrombectomy in a critically unwell patient with extensive PE who later underwent successful complex PCI.