
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-128
Severely Calcified Coronary Leading to Stent Deformity - Role of IVL Intra-Stent, A Stent Fracture and Bailout Thereof
By Rohit Mody
Presenter
Rohit Mody
Authors
Rohit Mody1
Affiliation
Mody Harvard Cardiac Institute & Research Centre, India1,
View Study Report
TCTAP C-128
Coronary - Complication Management
Severely Calcified Coronary Leading to Stent Deformity - Role of IVL Intra-Stent, A Stent Fracture and Bailout Thereof
Rohit Mody1
Mody Harvard Cardiac Institute & Research Centre, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 70 years old female, Came with Severe Chest pain, retrosternal with diaphoresis, ECG done showed ST-T changes and Trop-I was positive, Patient was diagnosed with Acute Coronary Syndrome, Patient's vitals were stable and patient was stable hemodynamically Diabetic, Hypertensive, Dyslipidemic, Obese, and Ejection Fraction- 45%


Relevant Test Results Prior to Catheterization
70 year old female, Diagnosed with ACS, Came with Severe Chest pain, Diabetic, Hypertensive, Dyslipidemic, Obese, Ejection Fraction- 45%
Relevant Catheterization Findings
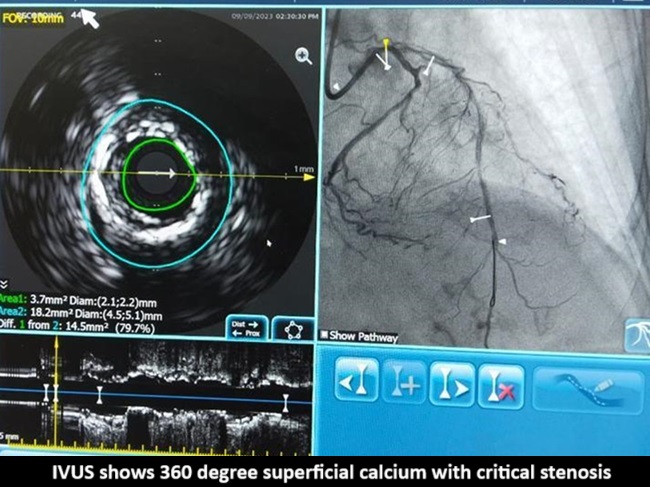
Angiogram shows calcified ostial Lad with critical stenosisLAD is showing calcified lesion from ostial to mid LAD separate origin of LADand LCX
Interventional Management
Procedural Step
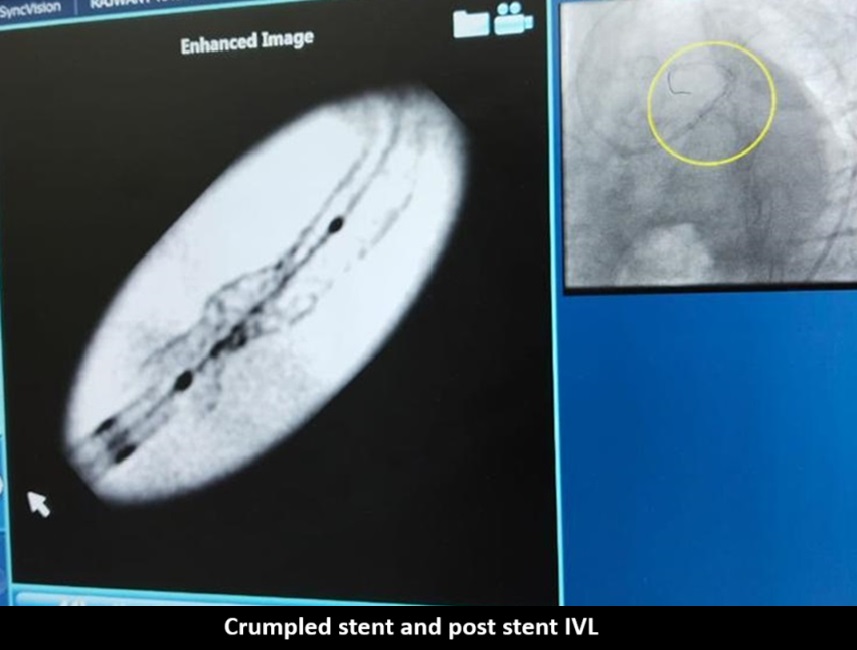
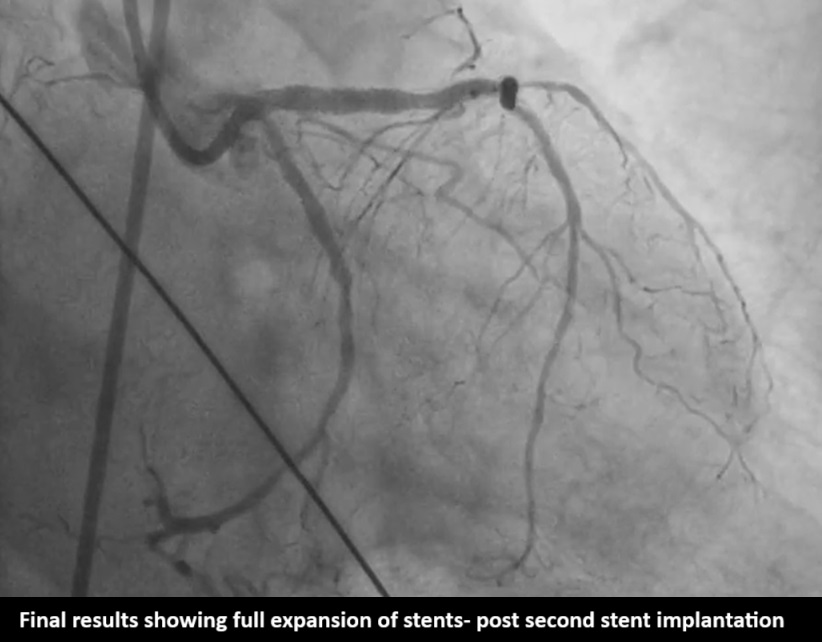
Pre PCI-IVUS showedsuperficial calcium 360 degree at ostium, Predilation was done with 2.5mm OPNballoon and 2.5 wolverine balloon, and 3.5x23mm (Xience Prime company) stentwas deployed at 18atm still there was severe dog boning and Crumpled stent canbe seen in Philips Sync Vision. 3.5x12 IVL done (shockwave company) with 8shocks each of 10 cycles within the crumpled portion Note inner dots containthe region of crumpled stent the way to position IVL for maximum strength. Post-inflationwith IVL, Stent fracture happened and a Clot started forming, another 3.5x23mm (BostonScientific Company) stent deployed in LAD with good result. After 2 hours inCCU patient suddenly developed chest pain and LVF, almost collapsed with BP40/20. Patient was started on inotropes, NIV support and ECG showed new onsetLbbb. It was thought that it could be SAT Gave additional heparin, Started onGp2 B. Fresh echo showed Rwma in LCX territory, new development. Put on IABP andShifted to Cathlab and a check angio done, Final angio with flowing LCX and LADPatient slowly weaned off NIV and IABP in further 3 days

Case Summary
In bedpreparation after predilating always do IVUS run post cutting balloon to see theeffect or take a bigger balloon to palpate. In our case we used 2.5 mm balloonto palpate but could not appreciate dog boning. Only after 3.5 stent we realizeddog boning. If stent iscrumbled can go with post stent IVL in our case after IVL stent expands butfractured and results in thrombus formation quickly another stent over it savedpatient on table. LCXdominant in our case and probably clot formed in it and lead to reMI and whenwe took to cathlab again it was flowing So remember as- Say always say lifenever ends till it really ends