
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-052
LM ACS With Shock, Comes Together With RCA CTO
By Detao Yan
Presenter
Detao Yan
Authors
Detao Yan1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-052
Coronary - Complex PCI - Left Main
LM ACS With Shock, Comes Together With RCA CTO
Detao Yan1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
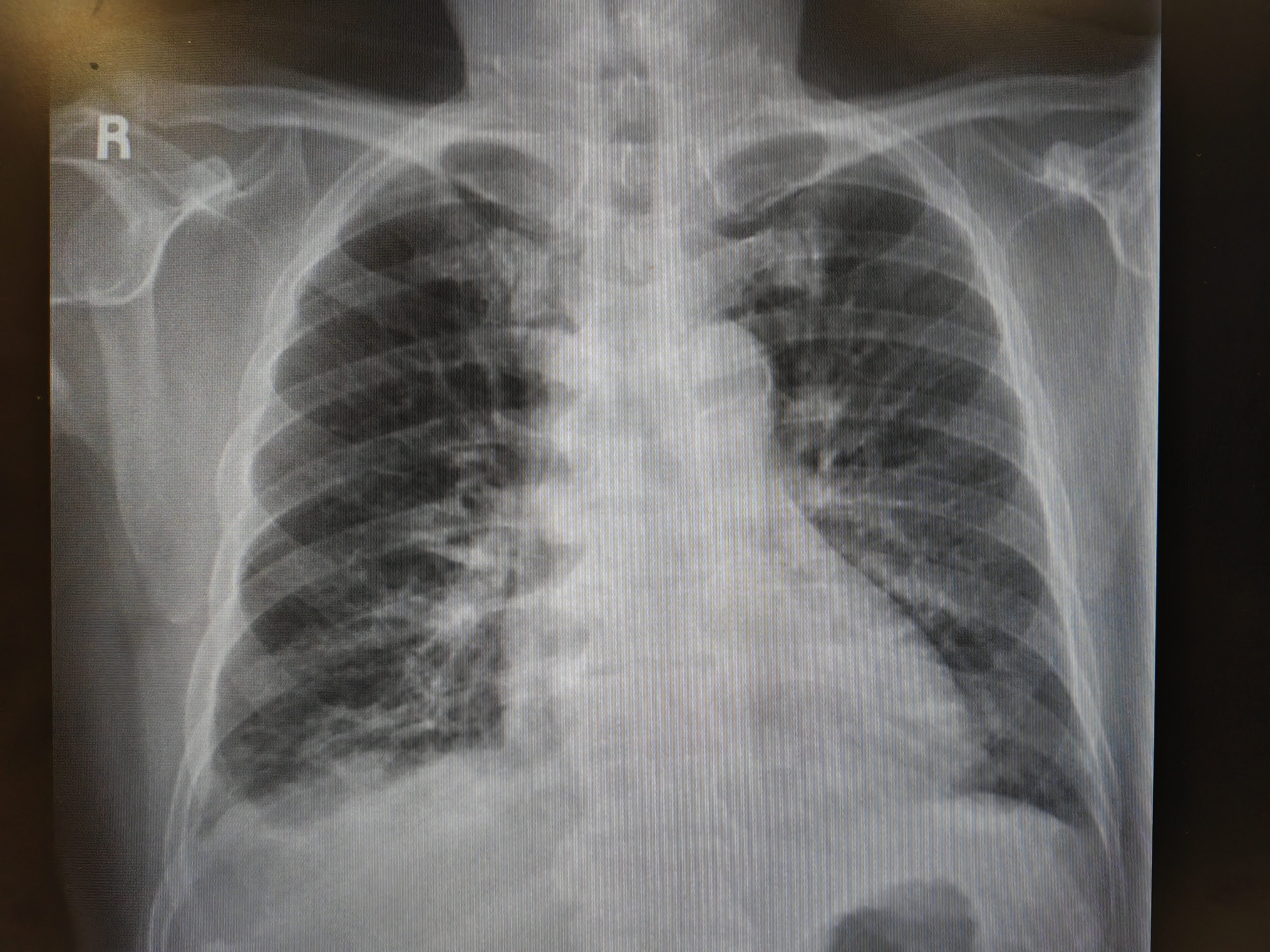
A 64-year-old gentleman with a history of diabetes, hypertension, hyperlipidemia presented to the emergency department with chest pain and dyspnea. Although initially hemodynamically stable with adequate oxygenation on 2L/min oxygen supplement, he soon developed desaturation and cardiogenic shock, requiring intubation with mechanical ventilation and inotropic support.
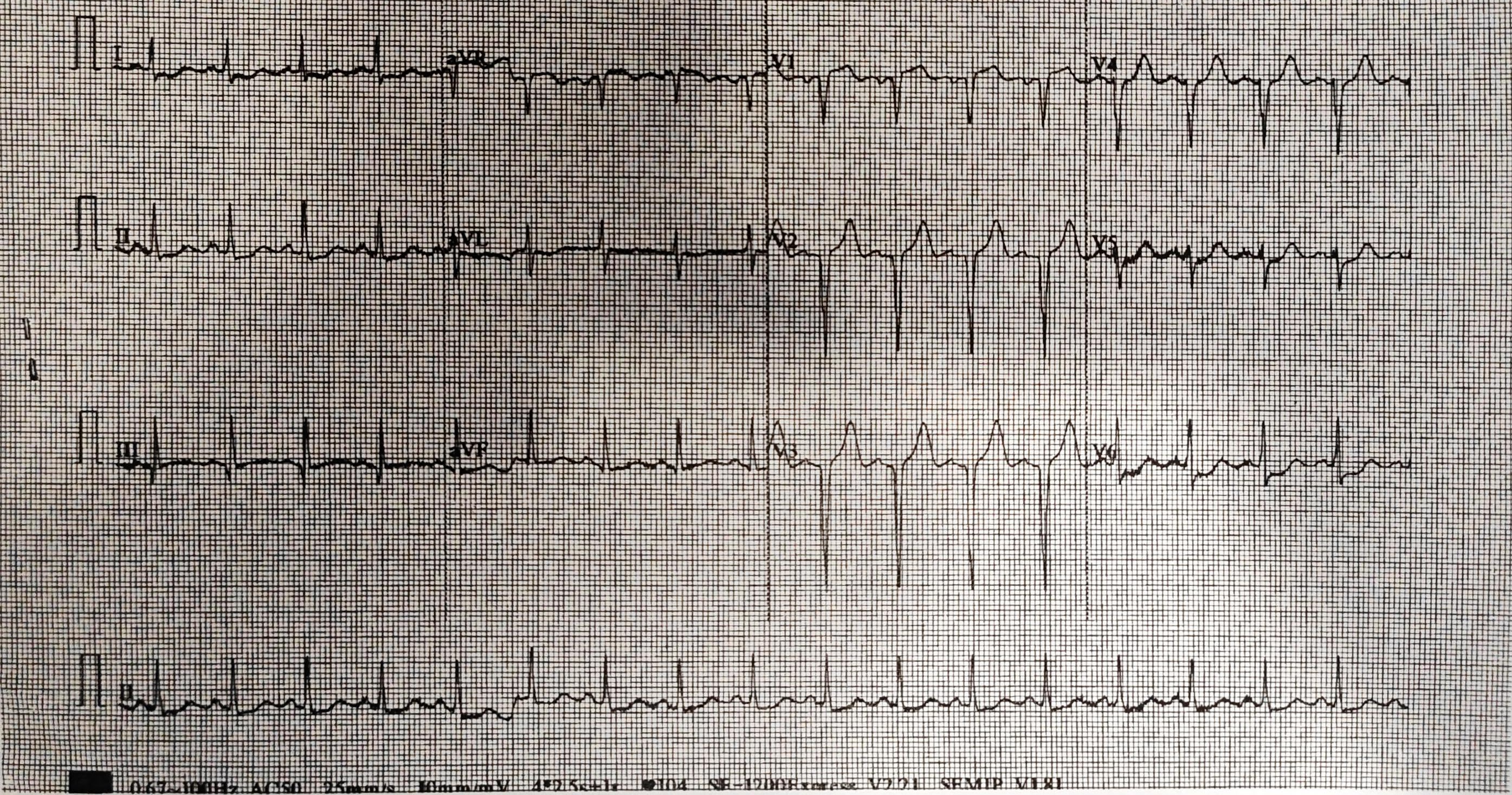
Relevant Test Results Prior to Catheterization
Chest X ray: pulmonary edema
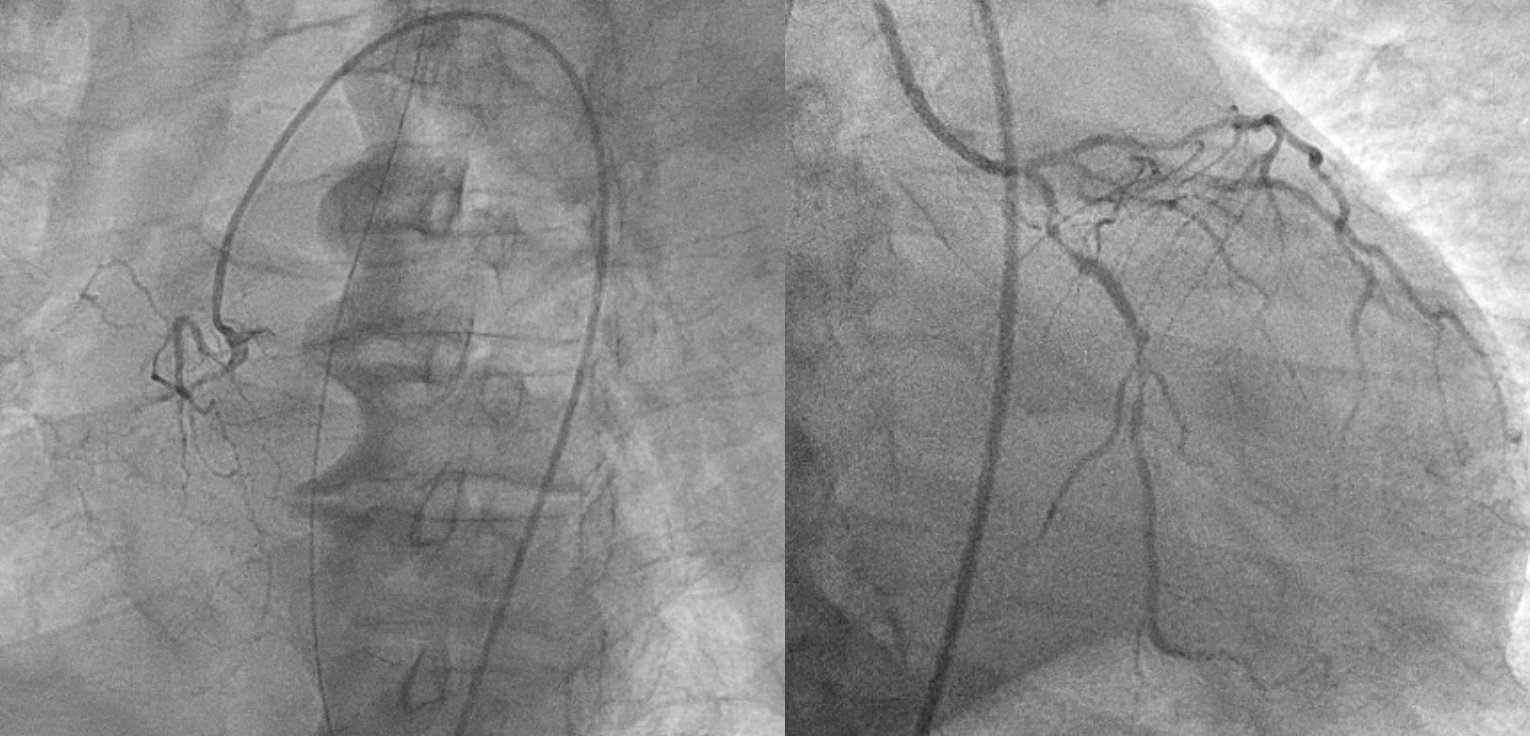
Relevant Catheterization Findings
Coronary angiography via right femoral approach with JL4 JR4 6Fr diagnostic catheters
Interventional Management
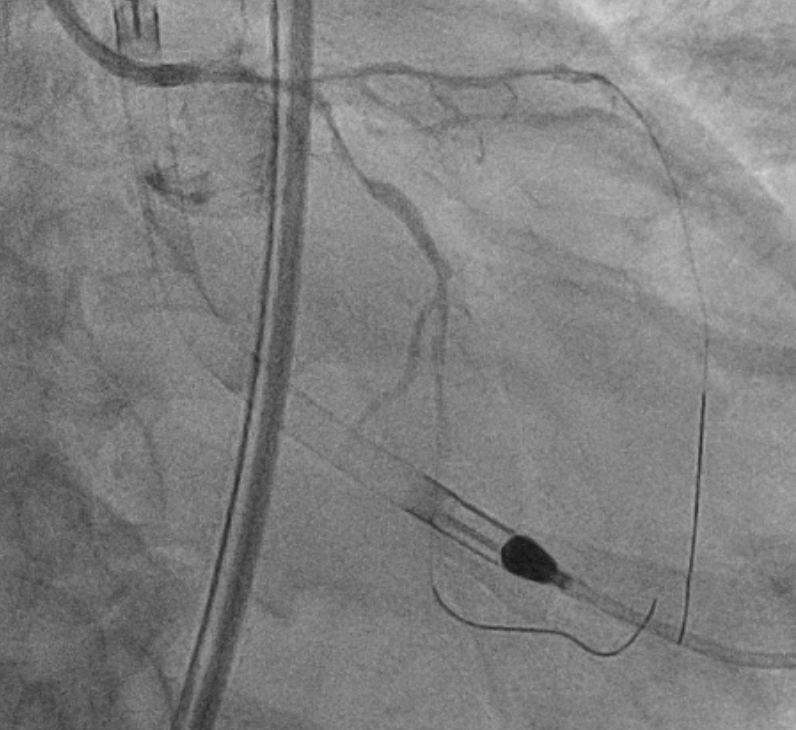
Procedural Step
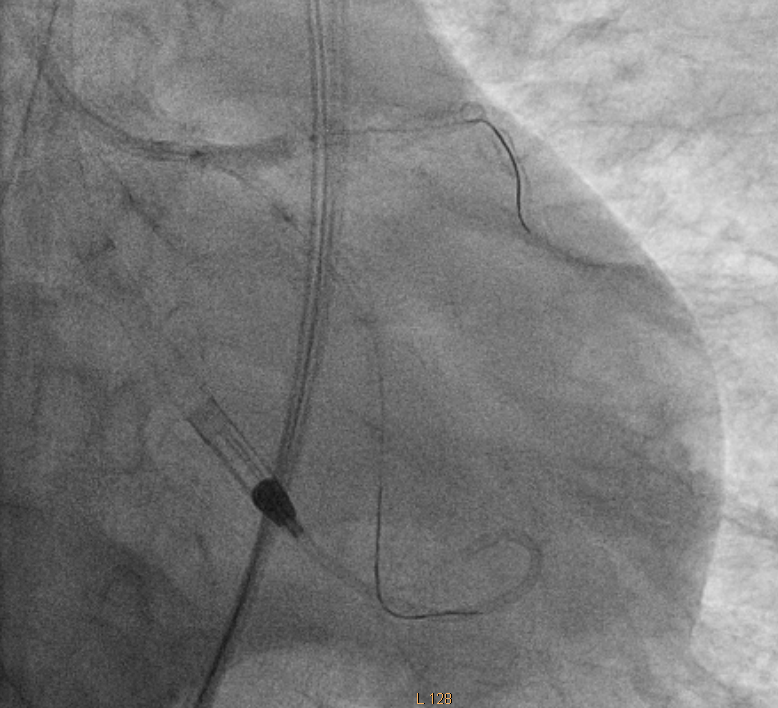
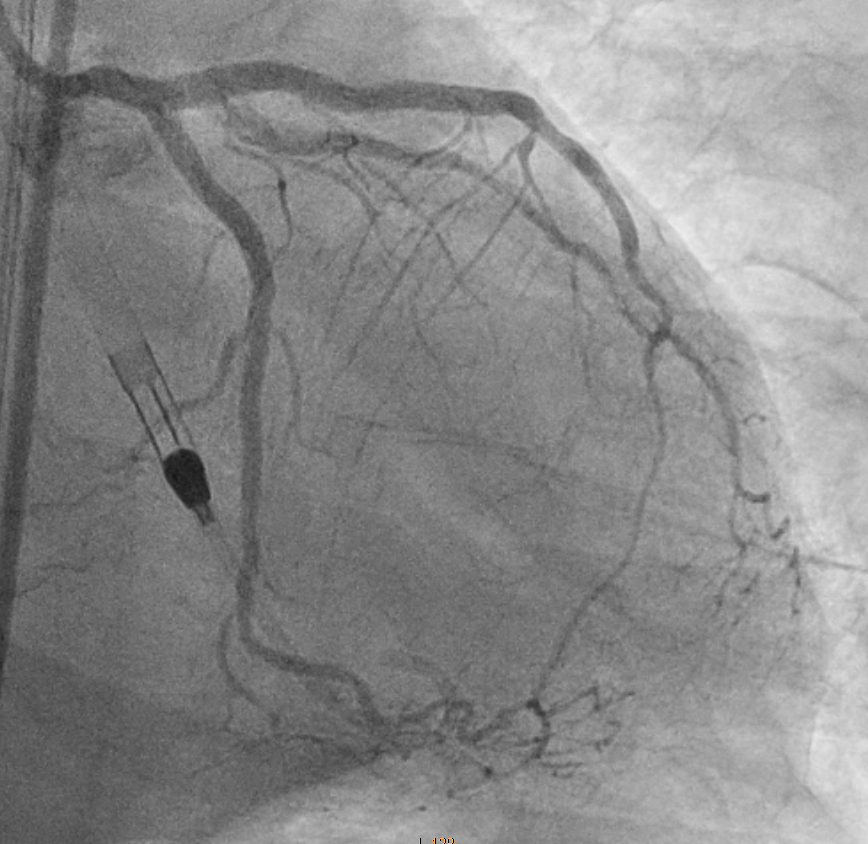
Impella CP was first placed for hemodynamic support. LM was engaged with JL 3.5 7Fr. dLCX and dLAD were then wired. LM-LCX was dilated with NC TREK 2.0/15 and NC Sapphire 3.0/15. o-mLCX was stented with Xience 2.0/33 and 2.75/23. The oLCX stent was then crushed with NC Sapphire 3.0/15. LM-oLAD was stented with Xience 3.5/23 and post-dilated with NC TREK 4.0/12. pLAD was pre-dilated with NC TREK 2.5/15 and NC Sapphire 2.75/12. The first diagonal branch (D1) was then wired, and pre-dilated with Sapphire 1.5/15 and NC Sapphire 2.0/15, then stented with Coroflex 2.0/16. pLAD was further pre-dilated and D1 stent crushed with Raiden 2.5/15 and Raiden 3.0/10. Then pLAD was again pre-dilated with NC TREK 3.5/15. p-mLAD was stented with Xience 2.5/38. Intravascular Ultrasound (IVUS) to LAD revealed stent under-expansion. LAD stents were then post-dilated with Raiden 3.0/10 and Raiden 3.5/10. LCX was rewired and stent strut opened with Zinrai 1.5/15. LCX stent was post-dilated with NC TREK 2.25/12, NC Sapphire 2.75/12 and Raiden 3.0/10. LAD/LCX kissing balloons were performed with NC TREK 3.5/15 and 3.0/15. LM proximal optimization technique (POT) was done with NC Pantera Leo 4.0/8. We then attempted to rewire D1 but unsuccessfully. We decided for staged percutaneous coronary intervention (PCI) to LAD/D1 bifurcation and RCA CTO in an outpatient setting, which was successfully performed later. The repeated echocardiogram showed an LVEF of 58% with no regional wall motion abnormalities.
Case Summary
Acute coronary syndrome (ACS) in the setting of LM bifurcation lesion is a challenging condition as it frequently results in cardiogenic shock. For this population, hemodynamic support during PCI is invaluable. While studies have compared the provisional 1-stent strategy versus a planned 2-stent strategy, patients with ACS are frequently underrepresented. Our case helps illustrate that: First, mechanical circulatory support with Impella CP during high-risk PCI is a complimentary approach. This is particularly relevant to our case as the patient also suffers from RCA CTO. Second, a planned 2-stent strategy is a feasible option for LM bifurcation PCI even in the setting of ACS.