
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-182
Patient With Polycythemia Vera Complicated by Severe Heart Failure
By Anuar Zhunussov
Presenter
Anuar Zhunussov
Authors
Anuar Zhunussov1
Affiliation
National Scientific Medical Center, Kazakhstan1,
View Study Report
TCTAP C-182
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Patient With Polycythemia Vera Complicated by Severe Heart Failure
Anuar Zhunussov1
National Scientific Medical Center, Kazakhstan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
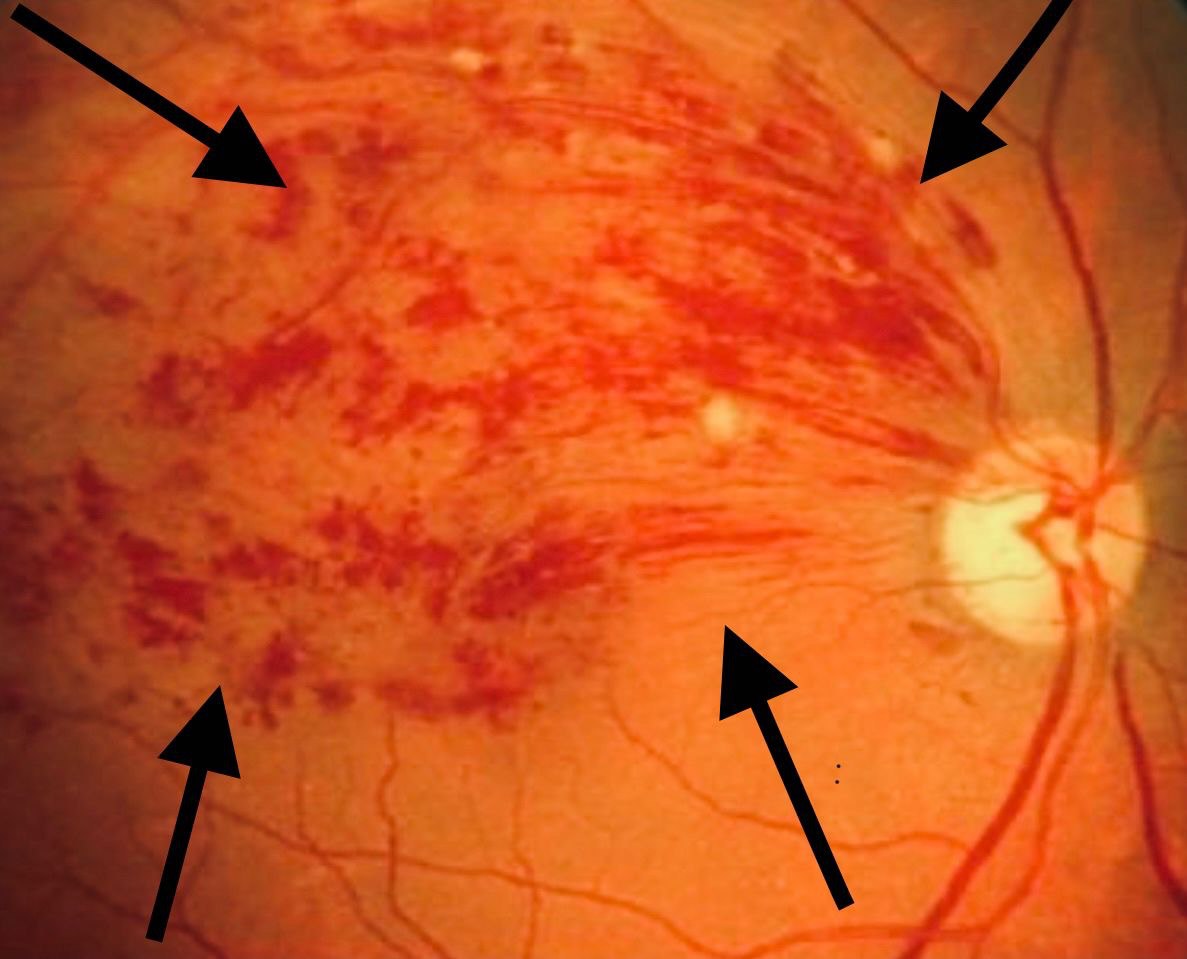
Patient E., age 57. From life history: At 39 years of age, acute thrombosis of the superior temporal central retinal vein of the right eye with successful treatment. In 2010, a coronary angiography with stenting of the LCx was performed. Then by genetic testing: JAK 2 gene mutation V617F, erythropoietin 4.5 IU/l. Diagnosis: Polycythemia Vera, JAK 2, V617F +, high risk of thrombosis. Was taking Hydroxycarbamide. But the appointment was performed irregularly.
Relevant Test Results Prior to Catheterization
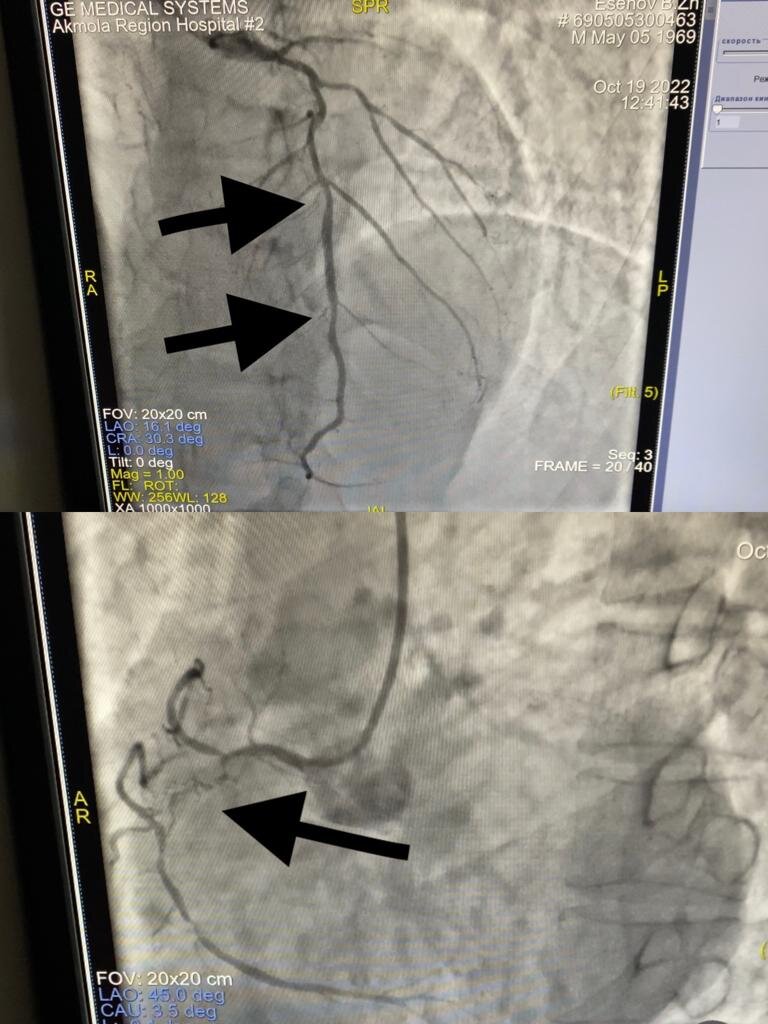
Coronary angiography: significant stenoses of the LAD and RCA. On examination: Right posterior tibial artery occlusion. EchoCG: multiple segmental akinesias. Left ventricular ejection fraction = 30 %. CBC: WBC- 17.20 x 109 /L; RBC - 7.01 x 1012 /L; HGB - 190.00 g/l; HCT - 56.10; PLT - 730.00 x 109 /L.
Relevant Catheterization Findings
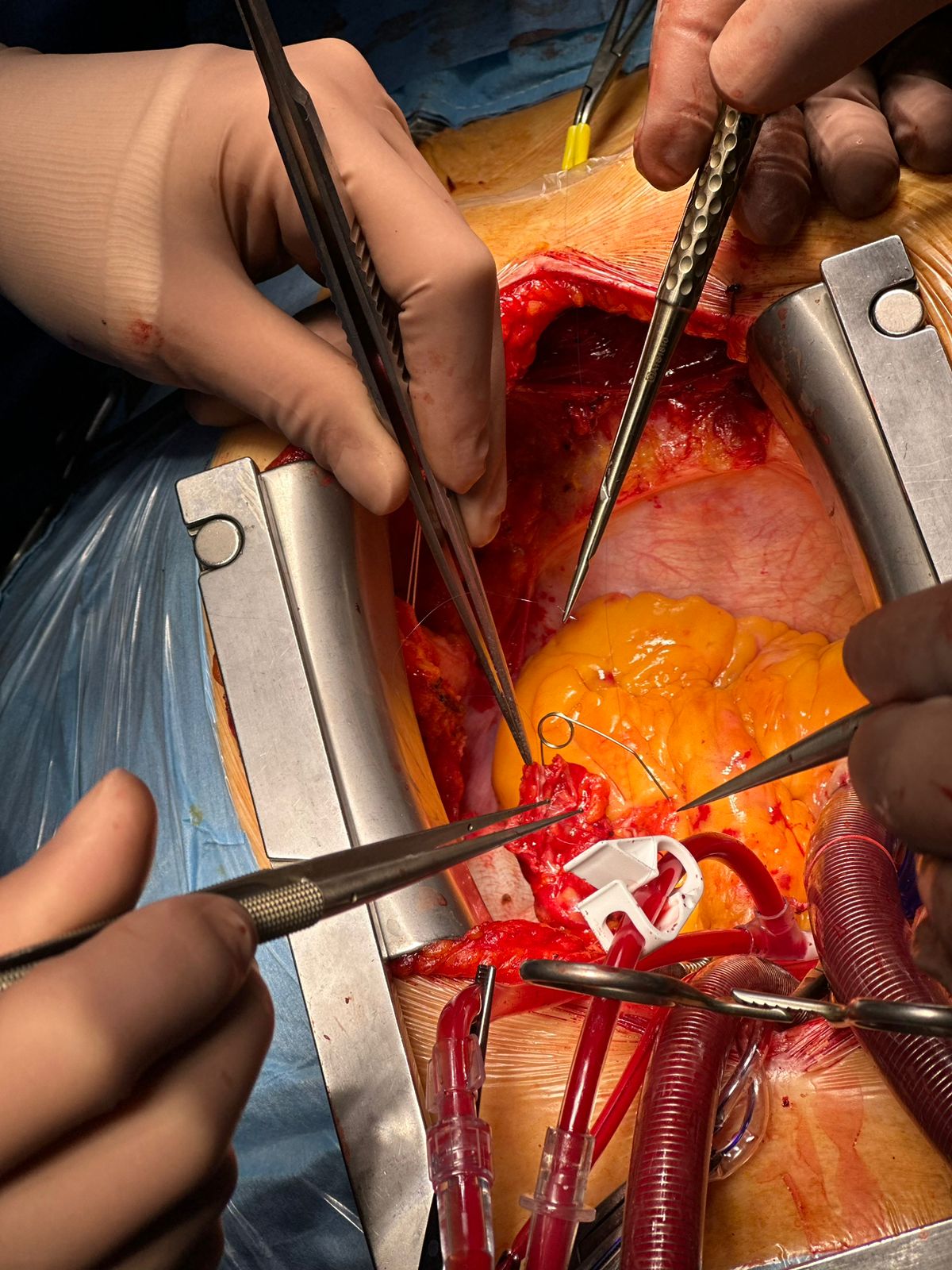
After examination by a cardiologist, hematologist, cardiac surgeon, and prescription of Hydroxycarbamide, surgery was performed: Aortocoronary bypass of LAD and RCA and therapy of heart failure.
Interventional Management
Procedural Step
Polycythemia Vera - Myeloproliferative disease. Complicated by vascular thrombosis of any localisation. Given the rarity of the disease, the tactics of managing such patients in cardiac surgery is not completely clear.This, after coronary artery bypass surgery, quality of life improved, echocardiography scores improved and the rise of sudden cardiac death decreased.In dynamics after 6 months CBC: Ht (41.1 %), PLT (393 x 109 /l), Leucocytes (6.6 x 109 /l). HGB 144.00 g/l. EchoCG: Left ventricular ejection fraction = 38 %. No recurrent thrombosis was observed.In a study by Abdykadyrov K.M. (2015), the proportion of Polycythemia Vera patients who had thrombosis (28 of 252) was 11.2 %, including 10 (3.6 %) patients with myocardial infarction and with heart failure. When haematocrit falls below 45 %, patients with Polycythemia Vera, after coronary artery bypass surgery, have a reduced risk of recurrent myocardial infarction, as our clinical example confirms. Taken together, this has a positive effect on the treatment of heart failure.
Case Summary
Diagnosing and treating Polycythemia Vera early prevents or reduces the risk of complications such as cardiovascular thrombosis. In case of complications with the development of heart failure, it is necessary to treat such patients together with hematologists, cardiologists and cardiac surgeons.