
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-153
Stent Disarticulation From the Ostium of the RCA
By Vinayak Nagaraja, Mohammad Sarraf
Presenter
Vinayak Nagaraja
Authors
Vinayak Nagaraja1, Mohammad Sarraf1
Affiliation
Mayo Clinic, USA1,
View Study Report
TCTAP C-153
Coronary - Complication Management
Stent Disarticulation From the Ostium of the RCA
Vinayak Nagaraja1, Mohammad Sarraf1
Mayo Clinic, USA1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
67 year old gentleman with previous PPCI to LCx 2012& CABG, PAF on Apixaban presents with acute pulmonary edema and ACS complicated by severe LV impairment. He treated with intravenous diuretics and guideline directed medical therapy.

Relevant Test Results Prior to Catheterization
His Iron deficiency anaemia was investigated with endoscopy and colonoscopy. This revealed inflammatory polyps with stigmata of recent bleeding treated with argon plasma coagulation. He was placed on sucralfate for 1 week and PPI therapy.

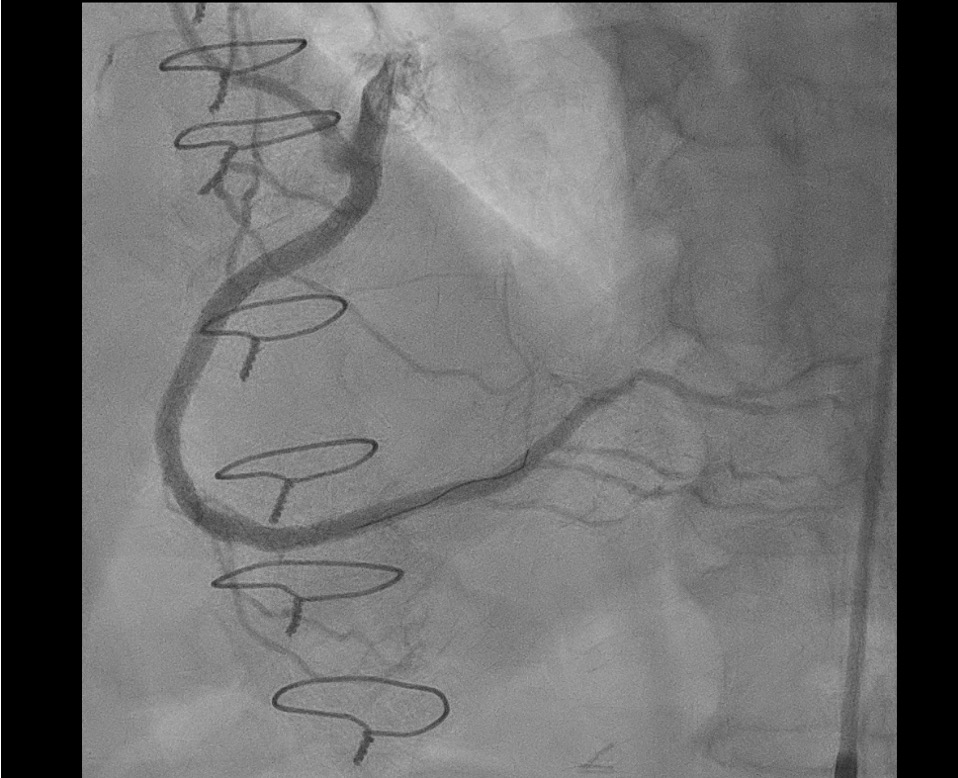
Relevant Catheterization Findings
His right study demonstrated normal filling pressures with normal cardiac output. His coronary angiography showed severe diffuse calcification of the RCA with an occluded graft. CMR demonstrated viability in the RCA territory. This was thought to be the target for revascularization.

Interventional Management
Procedural Step
We engaged the RCA with the 8Fr AL1 guide catheter. After administering heparin to a goal ACT of >250s, we advanced a sionblue coronary wire to the distal PLV using a Mamba flex microcatheter later swapped for a rotafloppy. We performed rotational arthrectomy was performed using a 1.5 mm Burr at 180K RPM with IV aminophylline. Later the rota floppy was replaced with a wiggle wire again. The vessel was prepared with multiple high pressure balloon inflations with a 3X20 NC balloon throughout the diffusely diseased vessel. The PDA was protected for a provisional one stent strategy. Afterwards using IVUS multiple DES were deployed in the RCA. The ostium of the RCA was dissected due to the guide catheter as demonstrated on IVUS. We placed a 4X38 Synergy at 14 atm in the ostium of the RCA that was placed inside the guide catheter extension.(Video 3) Later the stent balloon shaft fractured while removing the stent balloon. The plan was to get contralateral access and wire the dissected ostial vessel. Later removed the 8Fr system with a balloon anchor in the 8Fr guide and later snare the stent fragments using large one snare(35X120)(Video 4). Later a 3.5X32 Synergy megatron was placed in the ostium of the RCA at 16 atm later was post dilated with 5.0X12 NC balloon at 20 atm with an excellent result.


Case Summary
Lapses in focus during a long case can be due to fatigue. Focus on the deployment while you have a guide catheter extension. Snaring an important tool in an interventional cardiologist's arsenal. Maintaining wire access crucial across a dissection essential.