
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-233
Renal Artery Stenting Nightmare: When Innovation Saved the Day
By Ajay Joshi
Presenter
Ajay Joshi
Authors
Ajay Joshi1
Affiliation
Base Hospital, India1,
View Study Report
TCTAP C-233
Endovascular - Other Endovascular Intervention
Renal Artery Stenting Nightmare: When Innovation Saved the Day
Ajay Joshi1
Base Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
36 years old lady on 03 antihypertensive was detected of right renal stenosis. During renal artery stenting 7x15 renal stent migrated distal to the lesion and the second renal stent migrated proximally with a geographical miss. The proximal stent then embolized into aorta and was retrieved using novel technique with urology forceps flexible preventing an open procedure. In the same setting another 7X18 renal stent was overlapped with the distal stent and a satisfactory out come was achieved

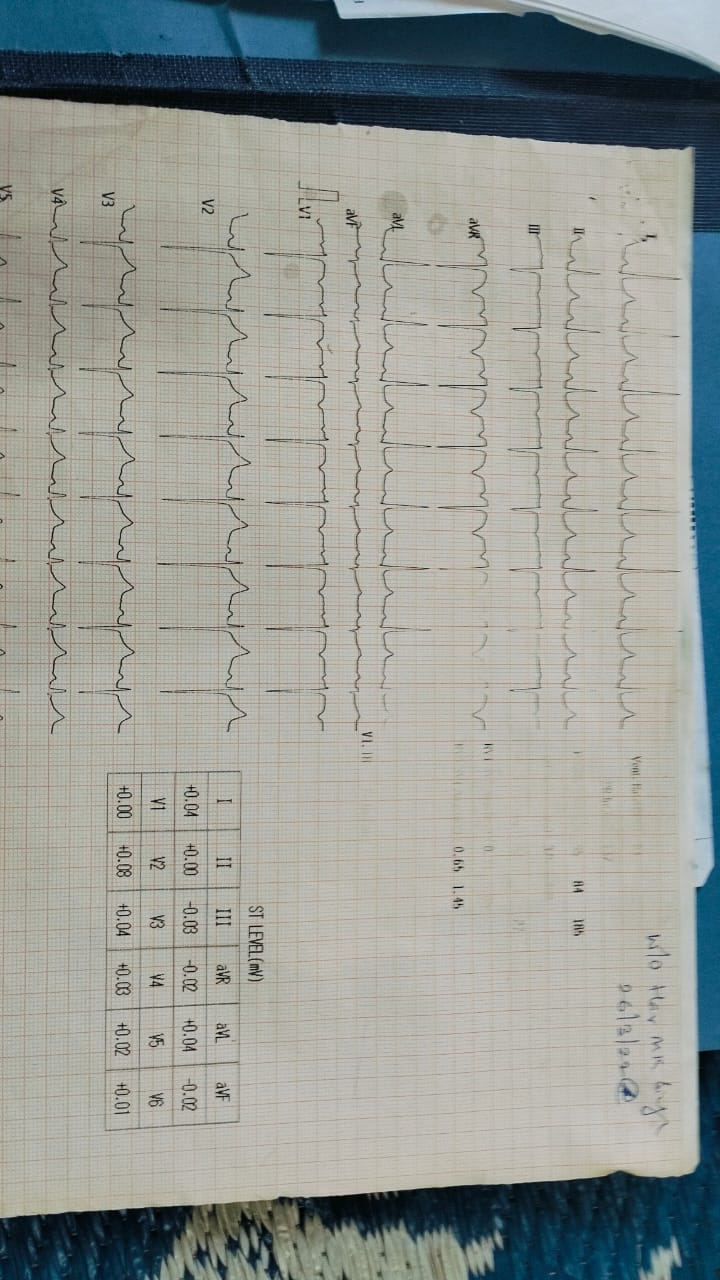
Relevant Test Results Prior to Catheterization
ECG shows LVH . on 2 D echo mild concentric LVH
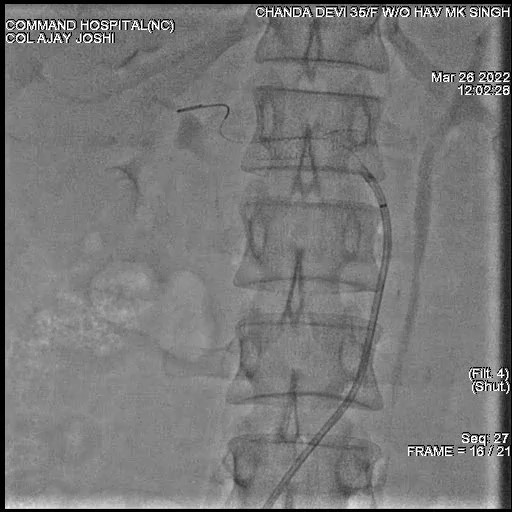
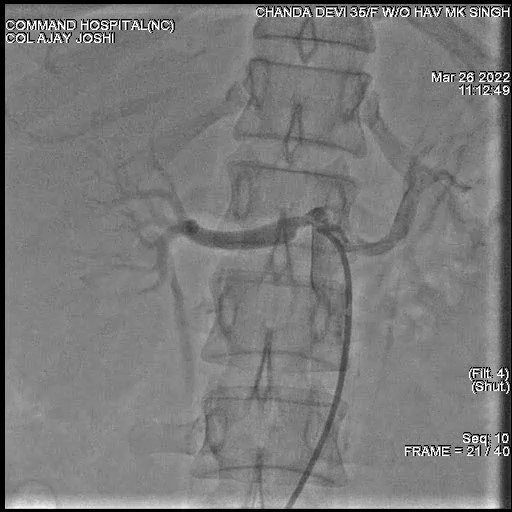
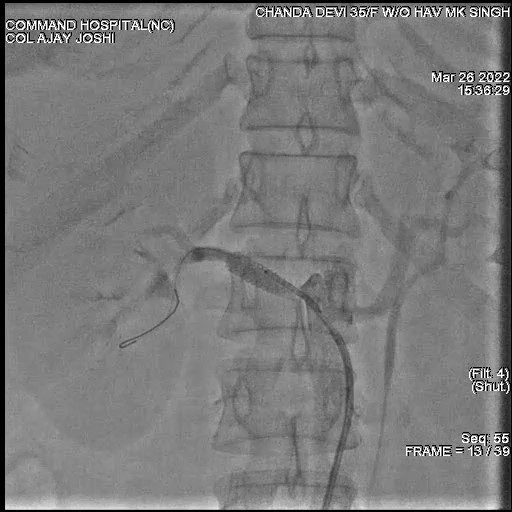
Relevant Catheterization Findings
on renal angiogram left renal artery normal, right renal artery stenosis, ostio - proximal 80% in AP, RAO 30 & LAO 30. likely atherosclerotic


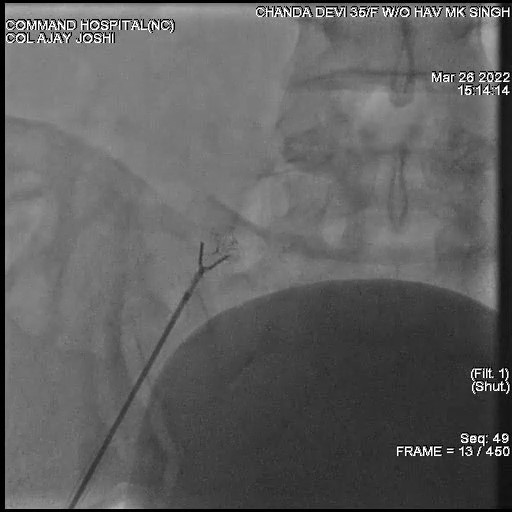
Interventional Management
Procedural Step
once the first stent migrated distal to stenosis the stent balloon was pulled back and no proximal pre-dilatation was done with the renal stent balloon . 6 X15 available renal stent also slipped proximally. BMW wire came out while negotiating third renal stent through 7 F renal guide . Rewiring with guidezilla support only managed to cross BMW wire from the side struts of stent and then the proximal renal stent dislodged back into the aorta and it reached the left external iliac artery. From the left femoral side, 7 F sheath was taken and an attempt was made to snare it out but it then migrated to right side. Many attempts were made with En snare ( life tech) of 3 F with loop diameter of 7mm and a buddy wire to snare it out , but they all failed. Even using a self made slit tip sheath did not work. Incidentally urology forceps had come to cath lab for ETO sterilization and the cath technician suggested to use it. On the other hand vascular surgeon called was eager for an open procedure. 5 F forceps flexible was taken across 7 F sheath into the right external iliac and without out much struggle the complete mangled renal stent was taken out from the sheath . A check shoot of both iliac artery was done, on finding no dissection a repeat right renal angiogram was done , following which a 7 x18 renal stent was negotiated and deployed across dissected angulated renal artery through a 7 F renal guide overlapping with the first renal stent with a satisfactory outcome.


Case Summary
Now after having this nightmare i call renal artery stenting a deceptively simple procedure. Appreciate the anatomy well of cephalic ,horizontal and caudal take off of renal arteries. Use cutting balloon and predilate. Renal stent balloon inflation should always be slow. During stent deployment there should be no undue forward or backward traction on the renal guide. Do not panic on renal stent dislodgement , keep different types of bail out snares ready. The innovative use of forceps flexible bailed me out from this difficult situation. 02 years post procedure she is on single antihypertensive ,normal urea creatinine and patent stents on contrast CT and renal angiogram