
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-070
Chip Revascularization With Mechanical Circulatory Support
By Jonathan Xinguo Fang
Presenter
Jonathan Fang
Authors
Jonathan Xinguo Fang1
Affiliation
National Heart Centre, Singapore, Hong Kong, China1,
View Study Report
TCTAP C-070
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Chip Revascularization With Mechanical Circulatory Support
Jonathan Xinguo Fang1
National Heart Centre, Singapore, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
JWP
Relevant Clinical History and Physical Exam
82-year-old man with history of hypertension and smoking presents with fall and sustained right hip fracture. Shortly after admission, he experienced chest pain. Cardiology was consulted by the orthopedic surgeon. Chest was clear on auscultation. There was a grade 3/6 pansystolic murmur at the apex. The jugular venous pressure was not elevated.


Relevant Test Results Prior to Catheterization
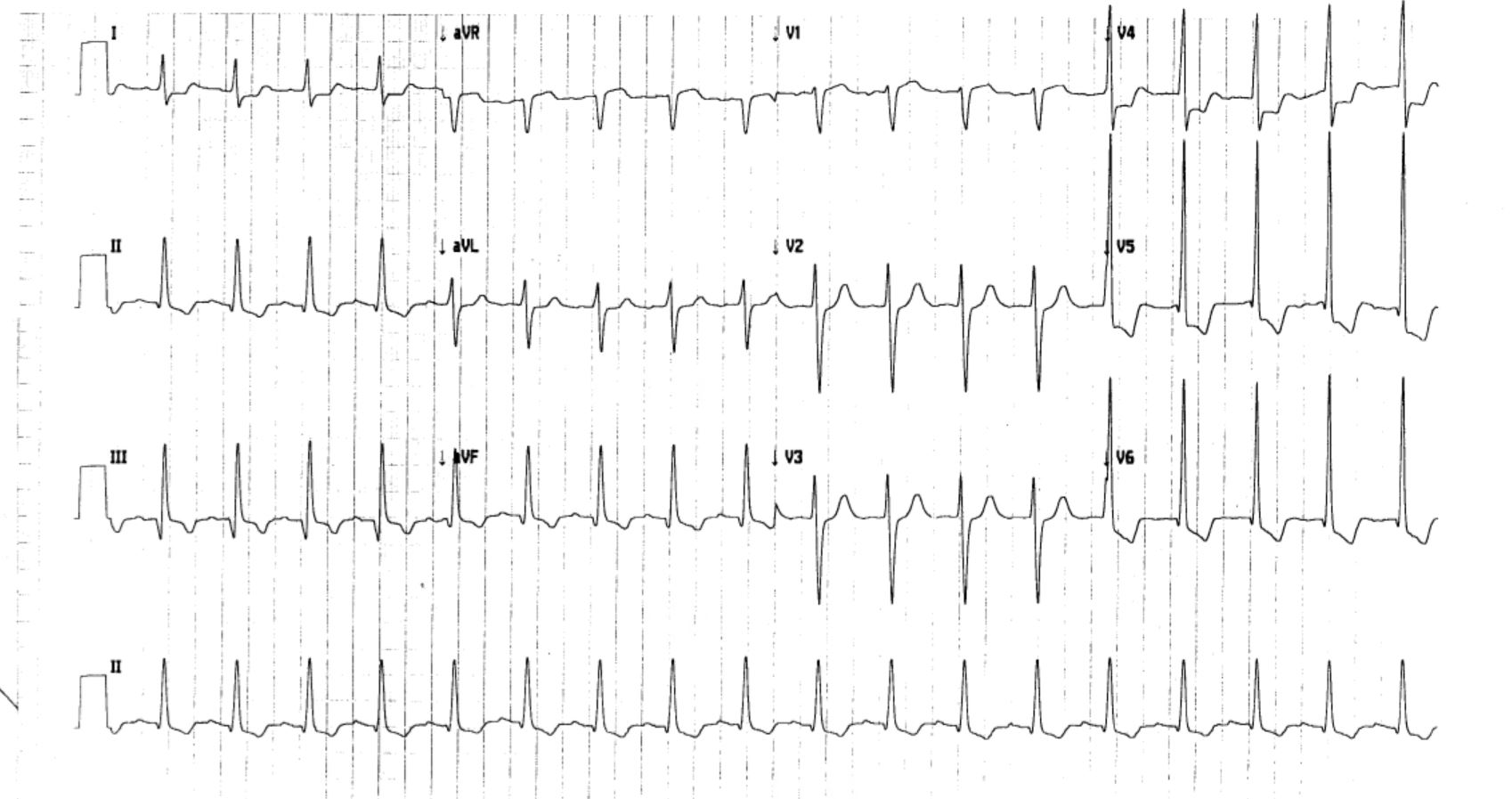
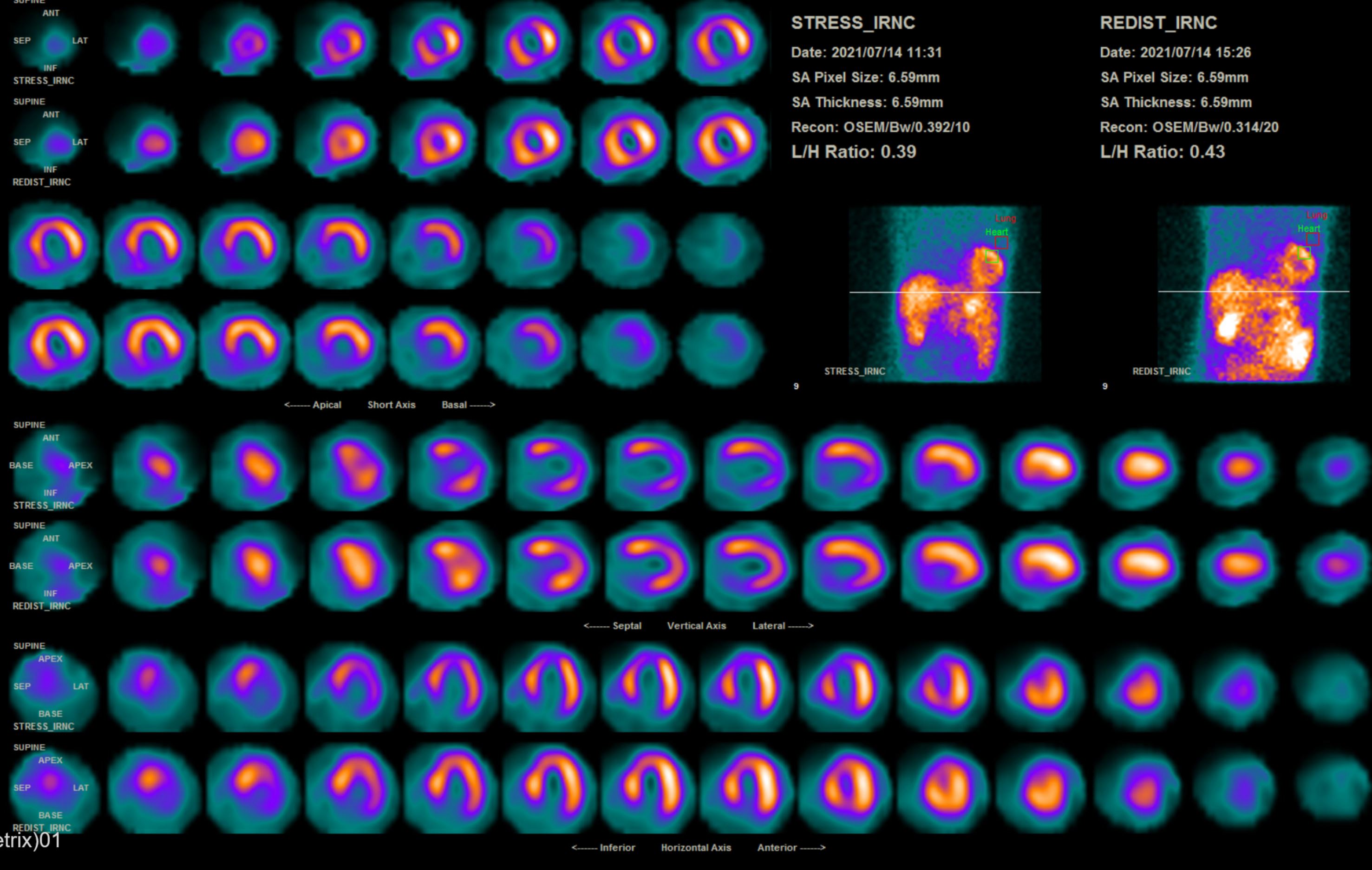
ECG showed inferior and lateral leads ST depression and aVR ST elevation.Echocardiogram showed global hypokinesia with EF 30~35%. Thallium scan showed viable myocardium with ischemia in anterior segments, inferior segments and apex.Chest x-ray showed clear lung fields.Right hip fracture was noted. Non-ST elevation acute coronary syndrome was diagnosed first.
 MOVIE-0036.avi
MOVIE-0036.avi
MOVIE-0037.avi
MOVIE-0038.avi
MOVIE-0039.avi
MOVIE-0040.avi
MOVIE-0041.avi
Relevant Catheterization Findings
RCA CTO. LAD aneurysmal
Left main coronary artery was heavily calcified with diffuse 60% disease. Left main-LAD-LCx showed Medina 1,1,1 disease. LAD showed heavily calcified 70-90% tortuous disease and aneurysmal change. D1 bifurcation showed 70% disease with m-dLAD with good target. Circumflex showed ostial 60-70% disease. OM1 and OM2 shows ostial 90% disease. Good target for CABG. RCA showed ostial 90% disease with pressure damping. Proximal RCA CTO with J-.
MOVIE-0028.mp4
MOVIE-0029.mp4
MOVIE-0030.mp4
MOVIE-0031.mp4
MOVIE-0032.mp4
MOVIE-0033.mp4
MOVIE-0034.mp4
MOVIE-0035.mp4
Left main coronary artery was heavily calcified with diffuse 60% disease. Left main-LAD-LCx showed Medina 1,1,1 disease. LAD showed heavily calcified 70-90% tortuous disease and aneurysmal change. D1 bifurcation showed 70% disease with m-dLAD with good target. Circumflex showed ostial 60-70% disease. OM1 and OM2 shows ostial 90% disease. Good target for CABG. RCA showed ostial 90% disease with pressure damping. Proximal RCA CTO with J-.
Interventional Management
Procedural Step
Left femoral access in view of right hip fracture. USG-guided puncture.
MOVIE-0042.mp4
MOVIE-0044.mp4
MOVIE-0046.mp4
MOVIE-0050.mp4
MOVIE-0051.mp4
MOVIE-0052.mp4
MOVIE-0064.mp4
MOVIE-0070.mp4
MOVIE-0085.mp4
MOVIE-0087.mp4
MOVIE-0095.mp4
MOVIE-0102.mp4
MOVIE-0108.mp4
MOVIE-0111.mp4
MOVIE-0112.mp4
MOVIE-0114.mp4
Preclose with 2 proglide. 14 French sheath and Impella CP.
PCI to RCA CTO
7 French AL 0.75 guide. JL4 diagnostic for contralateral injection
Turnpike 135 with Fielder XTA followed by Gaia 2nd antegrade wire escalation to RCA true lumen. Exchange to Sion Blue. Balloon with 2.0 balloon. Further balloon with NC scoreflex 2.5. Stent with Resolute Onyx 2.5/38 , 3.0/26, 3.5/22. Postdialte with NC 3.5 at 20 atm and NC 4.0 at 16 atm
mRCA postdilate with NC 3.0 and 2.5 balloon at 22 atm. distal stent edge dissection noted, stented with Resolute Onyx 2.5/18.
PCI to LM-LAD. Rotablation with 1.5 burr at 180000 rpm 8 passes, 1.75 burr at 170000 for 3 passes. Exchange to Sion Blue wire. Runthrough NS wire to LCx.
IVUS done to LM-LAD and LCx showed aneursymal disease and calcification.
LM-LAD dilated with NC Scoreflex 2.5, stent with Resolute Onyx 2.75/35. LM-LAD stent with Resolute Onyx 3.5/34. POT with NC 4.0 at 16 atm. LAD post dilate with NC 3.0 at 22 atm, NC 3.5 at 16 atm. IVUS and angiograms showed good result. Impella weaned and wound closed with Perclose x 2.
Case Summary
Complex PCI with Impella support in high-risk indicated patient can be life-saving with careful procedural planning and case selection. In this patient with ACS and hip fracture, timely revascularization is crucial. In this patient, despite coronary revascularization, the hip fracture was managed conservatively. The hip healed with malunion. Nevertheless, the patient was able to go under rehabilitation program and regain some of his mobility and weight-bearing. Today he can walk with a frame.