
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-149
Contrast Utilization During Chronic Total Occlusion Intervention
By A.A. Sg. Mas Meiswaryasti Putra, Doni Firman, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom
Presenter
A.A. Sg. Mas Meiswaryasti Putra
Authors
A.A. Sg. Mas Meiswaryasti Putra1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-149
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
Contrast Utilization During Chronic Total Occlusion Intervention
A.A. Sg. Mas Meiswaryasti Putra1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Mr. AR
Relevant Clinical History and Physical Exam
The patient came with chief of complain: angina on effort. He had history of NSTEMI TIMI 6/7, GRACE 132, CRUSAD 43 about 2 months ago (09/2020), early CAG was done with results CAD2VD + CTO LAD. The Heart Team decided to do PCI at LAD. He had several risk factor for CAD: hypertension and DM type II on routine medication. The physical examination was remarkable.
Relevant Test Results Prior to Catheterization
ECG : SR, HR 89 bpm, Q wave at at lead II and III, ST depression at V5-V6, I, aVLECHOCARDIOGRAPHY : EF by Simpson 55%, global normokinetic , TAPSE 24 mm, all valves normal
Relevant Catheterization Findings
Early CAG 20/09/20 :LM : NormalLAD : Moderate-severe calcification at proximal, CTO at proximal, distal had flow from contralateral (Rentrop 3)LCx : Irreguler di proximal,OM3: Stenosis 80-90%RCA : Dominan, 50-60% stenosis at proximal
Interventional Management
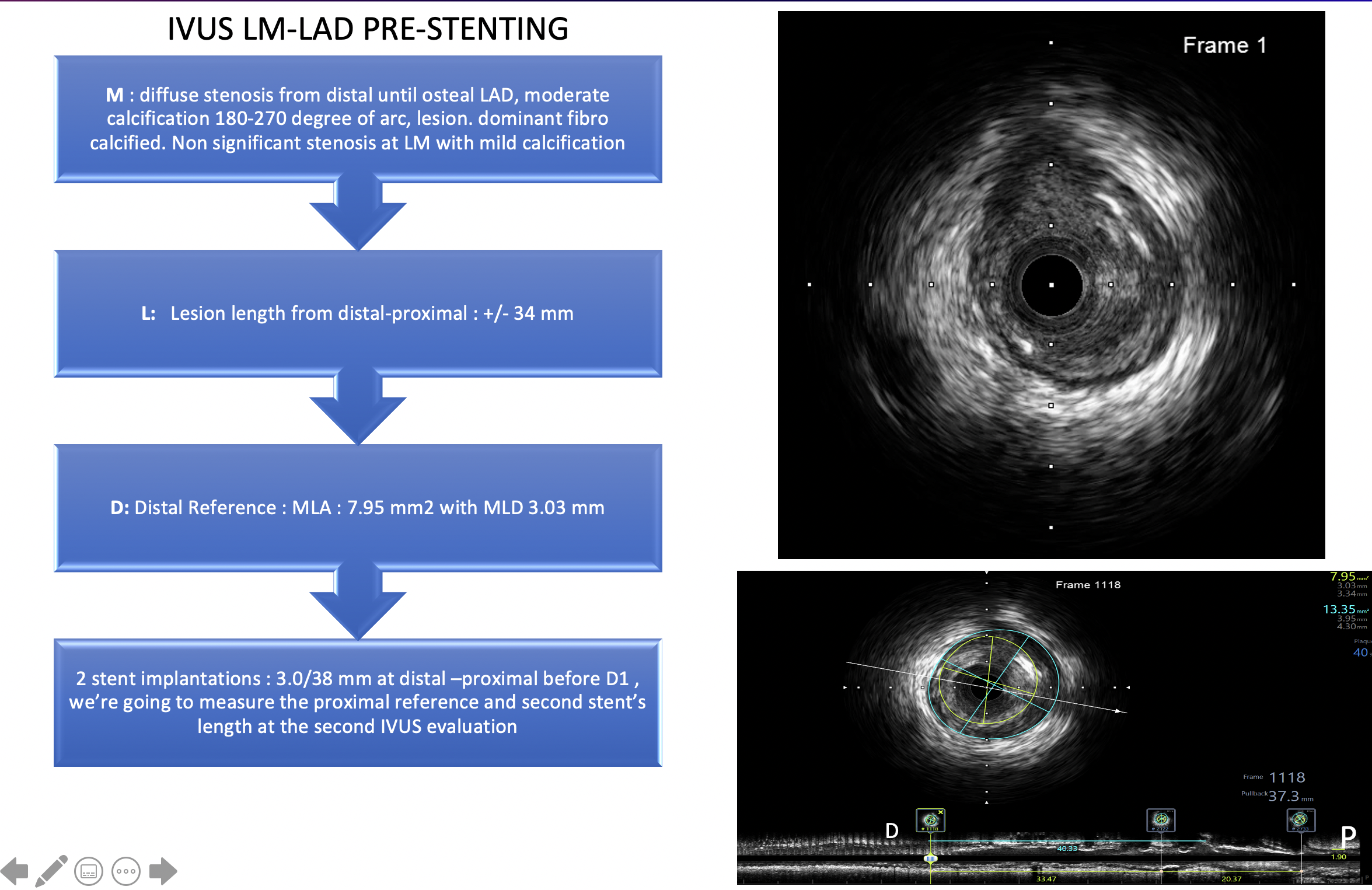
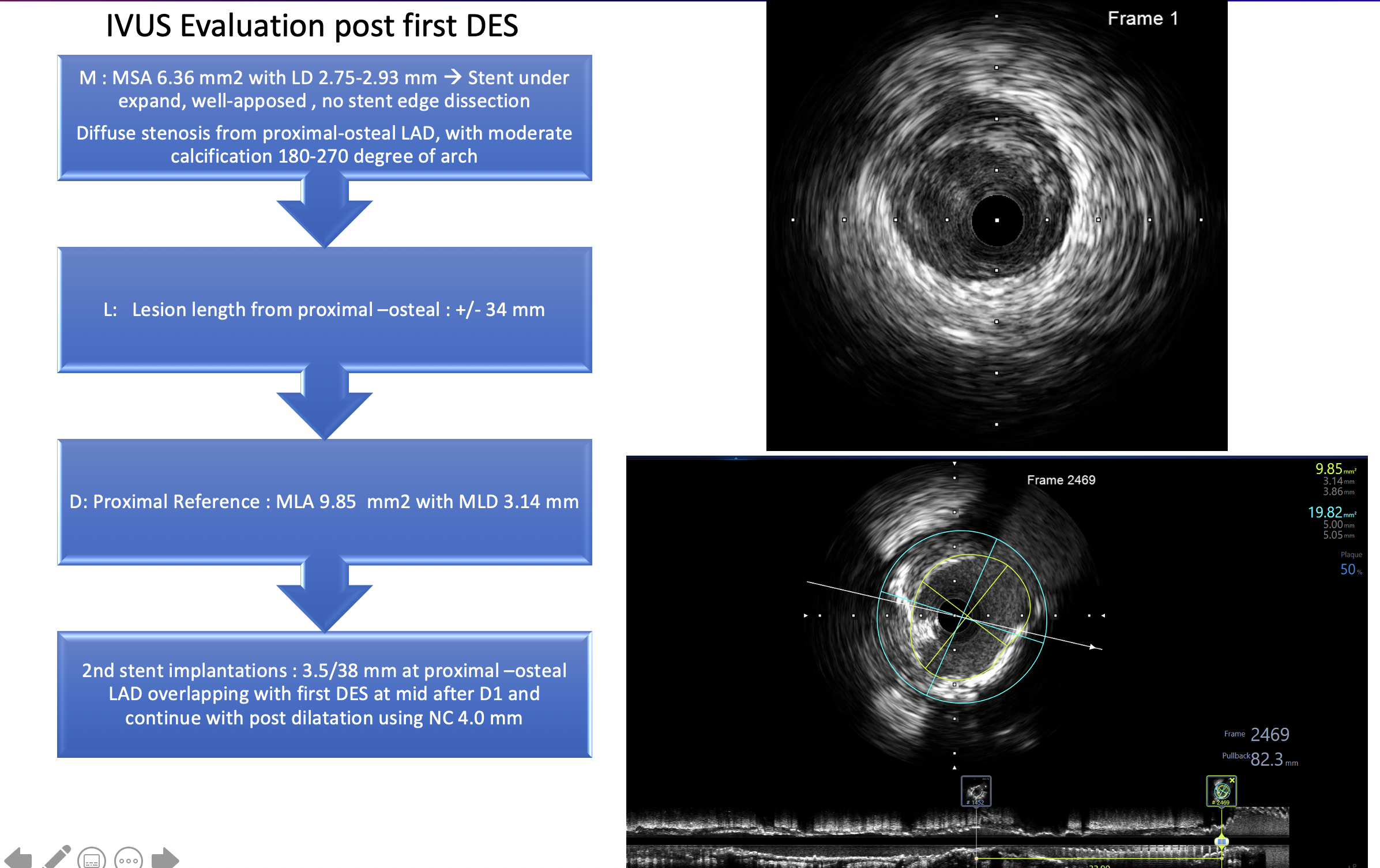
Procedural Step
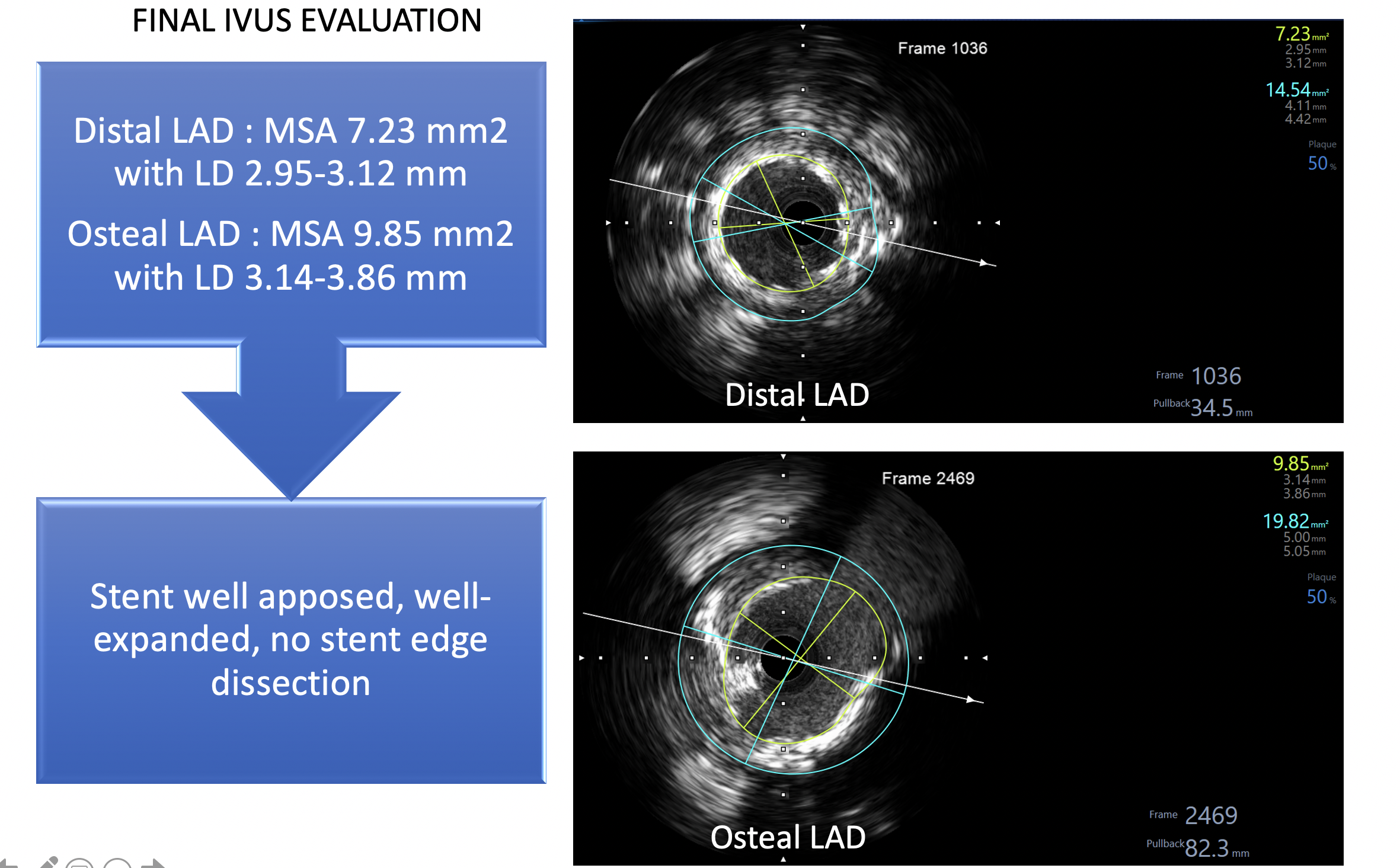
Using GC : XB 3.5/7F. Succesfully crossing CTO with Asahi Fielder XT-A back up microcatheter Finecross 1.8F. Exchange Fielder XT-A with Runthrough Floppy NS and double wiring to D1 with Runthrough NS. Predilatation : SC Ryujin 2.0/15 mm distal-proximal LAD. IVUS with Opticross 3F imaging catheter to distal LAD, and auto pullback. Based on IVUS results, we planned to do 2 stent implantations: 3.0/38 mm at distal –proximal before D1 , we’re going to measure the proximal reference and second stent’s length at the second IVUS evaluation. First DES Promus Premier 3.0/38 mm with high pressure at distal-proximal LAD before D1. Second IVUS evaluation was done and second DES Promus Premier 3.5/38 mm at prox-osteal LAD implanted overlapping with first DES at mid after D1. Post dilatation NC Treks 4.0/12 mm. Final IVUS : Stent well apposed, well-expanded, no stent edge dissection. Final Angio: TIMI 3 flow, thrombus (-), dissection (-). Total contrast : 20 cc
Case Summary
IVUS as a primary imaging tool to guide PCI was safe and markedly reduced the volume of iodine contrast as compared with angiography-guided PCI. Contrast utilization during CTO intervention is important to reduce the risk of CIN especially in patients with renal impairment.